Welcome to China Oncology,
China Oncology ›› 2025, Vol. 35 ›› Issue (5): 449-456.doi: 10.19401/j.cnki.1007-3639.2025.05.003
• Original article • Previous Articles Next Articles
YING Leilei( ), LI Kening, CHEN Chao, WANG Ying, HUANG Haozhe, WANG Biao, LI Wentao, HE Xinhong()
), LI Kening, CHEN Chao, WANG Ying, HUANG Haozhe, WANG Biao, LI Wentao, HE Xinhong()
Received:2025-03-25
Revised:2025-05-09
Online:2025-05-30
Published:2025-06-10
Contact:
HE Xinhong
Supported by:Share article
CLC Number:
YING Leilei, LI Kening, CHEN Chao, WANG Ying, HUANG Haozhe, WANG Biao, LI Wentao, HE Xinhong. Impact of tumor diameter on post-radiofrequency ablation survival and local progression risk in patients with colorectal cancer lung metastasis[J]. China Oncology, 2025, 35(5): 449-456.
Fig. 1
Flowchart of patient inclusion and exclusion"
Tab. 1
Clinical characteristics of patients enrolled [n (%)]"
| Characteristic | Total (n=134) | Small group (n=77) | Large group (n=57) | P value |
|---|---|---|---|---|
| Age/year $\bar{x} \pm s$ | 59.3±12.1 | 57.6±11.7 | 60.3±12.3 | 0.226 |
| Gender | 0.714 | |||
| Female | 54 (40.3) | 30 (39.0) | 24 (42.1) | |
| Male | 80 (59.7) | 47 (61.0) | 33 (57.9) | |
| Location | 0.494 | |||
| Left | 73 (54.5) | 40 (51.9) | 33 (57.9) | |
| Right | 61 (45.5) | 37 (48.1) | 24 (42.1) | |
| Number of lesions | 0.833 | |||
| 1 | 107 (79.9) | 61 (79.2) | 46 (80.7) | |
| 2 | 27 (20.1) | 16 (20.8) | 11 (19.3) | |
| Extrapulmonary metastatic | 0.62 | |||
| None | 89 (66.4) | 53 (68.8) | 36 (63.2) | |
| Exist | 45 (33.6) | 24 (31.2) | 21 (36.8) | |
| Preoperative CEA/(ng·mL-1) | 0.601 | |||
| <5 | 69 (51.5) | 39 (50.6) | 30 (52.6) | |
| ≥5 | 65 (48.5) | 38 (49.4) | 27 (47.4) |
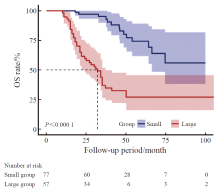
Fig. 2
OS rate curves of CRC patients with pulmonary metastases of different tumor diameters after RFA"
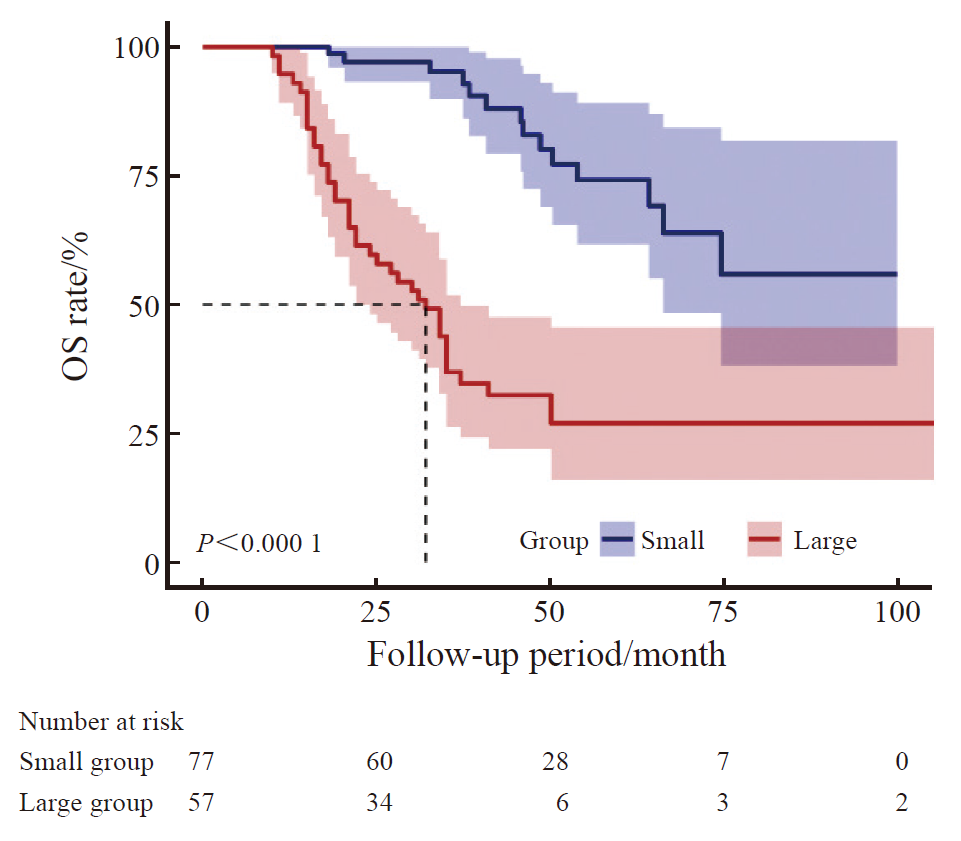
Fig. 3
PFS rate curves of CRC patients with pulmonary metastases of different tumor diameters after RFA"
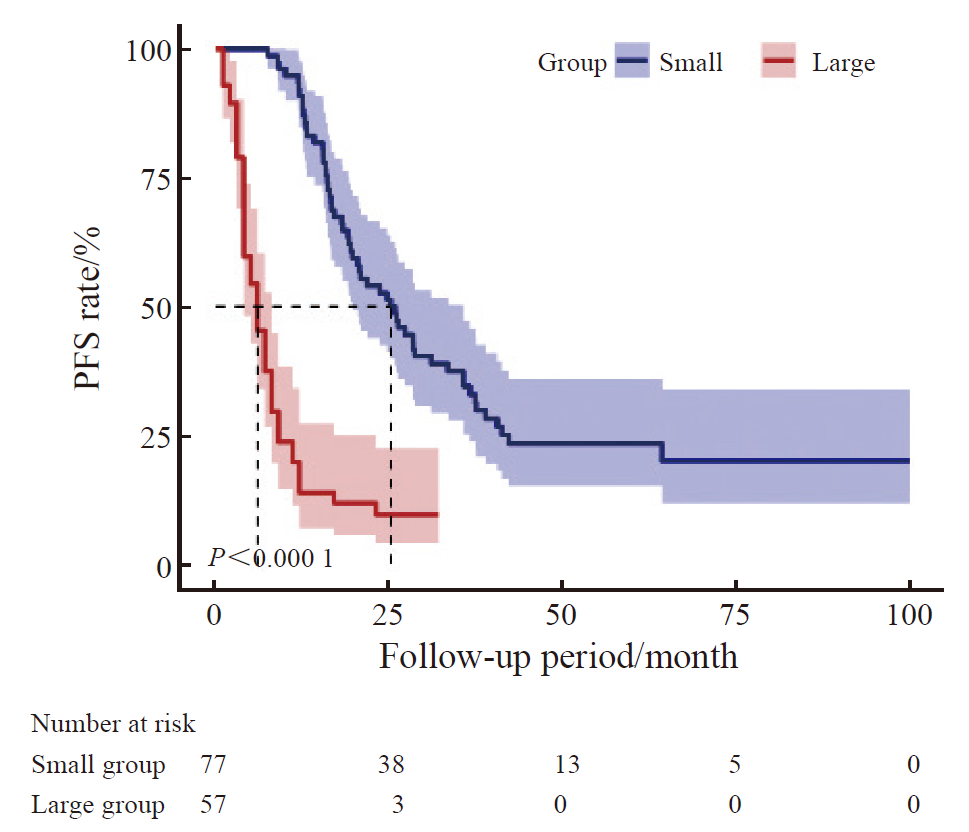
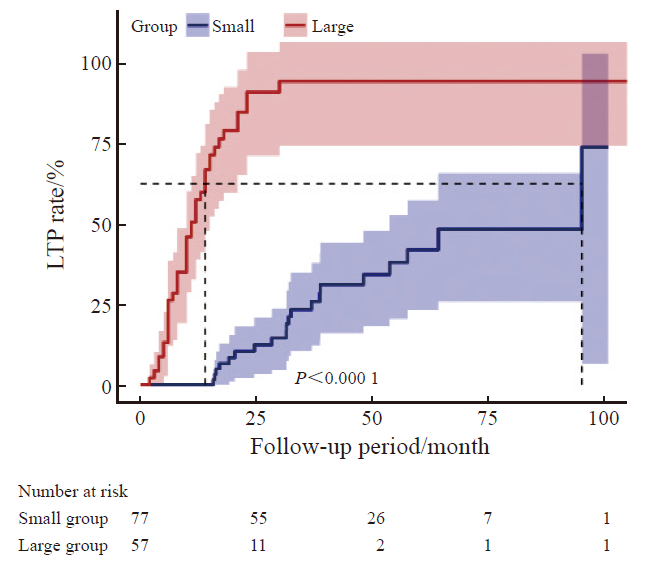
Fig. 4
LTP rate curves of CRC patients with pulmonary metastases of different tumor diameters after RFA"
Tab. 2
Univariate analysis of the correlation between RFA and OS in CRC patients with lung metastases"
| Variable | β (95% CI) | P value |
|---|---|---|
| Age | 1.01 (0.99, 1.04) | 0.280 |
| Gender | 0.366 | |
| Female | 1 (reference) | |
| Male | 0.78 (0.45, 1.34) | |
| Location | 0.849 | |
| Right | 1 (reference) | |
| Left | 0.95 (0.55, 1.63) | |
| Diameter | 1.96 (1.55, 2.48) | <0.001 |
| Preoperative CEA/(ng·mL-1) | 0.033 | |
| <5 | 1 (reference) | |
| ≥5 | 1.82 (1.05, 3.17) | |
| Extrapulmonary metastasis | 0.298 | |
| None | 1 (reference) | |
| Exist | 1.26 (0.81, 1.96) | |
| Number of lesions | 0.300 | |
| 1 | 1 (reference) | |
| 2 | 0.66 (0.29, 1.46) |
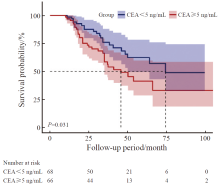
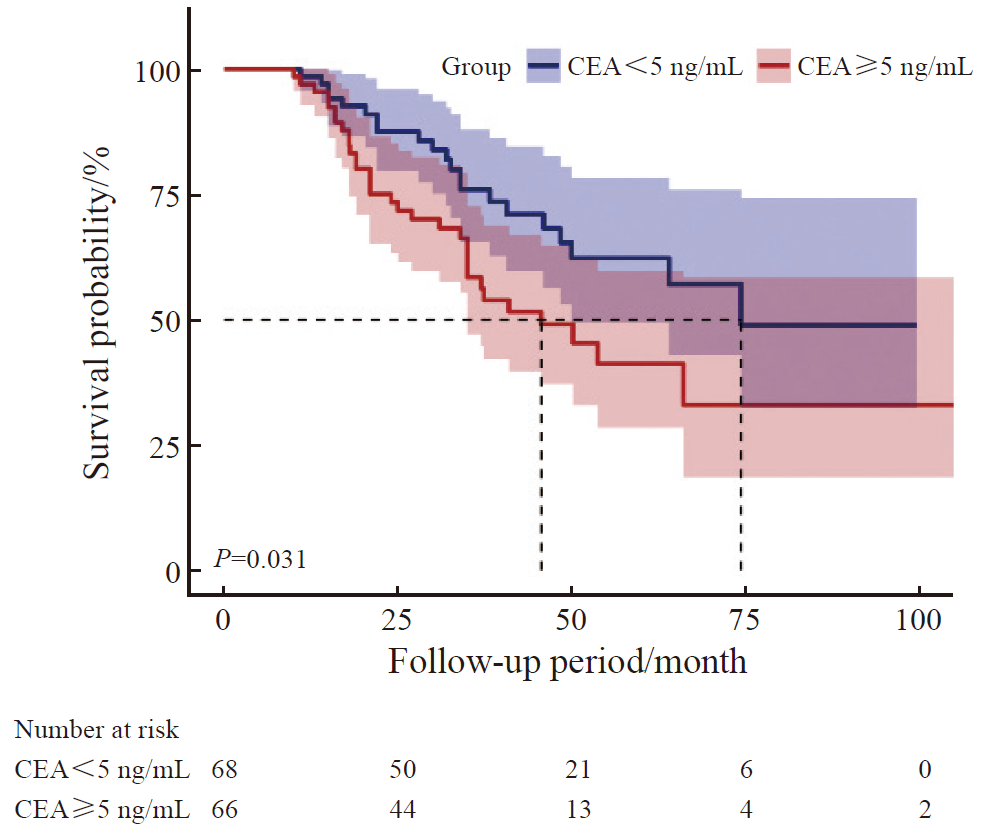
Fig. 5
Survival curves of CRC patients with lung metastasis after RFA treatment stratified by preoperative CEA levels"
Tab. 3
Multivariable COX regression analysis of the correlation between different tumor diameters and OS in patients with CRC pulmonary metastases following RFA"
| Group | Total | Event | Crude | Model-1 | Model-2 | Model-3 |
|---|---|---|---|---|---|---|
| Small | 77 | 14 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Large | 57 | 39 | 5.7 (3.06-10.6) | 5.84 (3.09-11.05) | 6.39 (3.34-12.21) | 6.49 (3.18-13.24) |
| P value | <0.001 | <0.001 | <0.001 | <0.001 |
| [1] | BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024, 74(3): 229-263. |
| [2] | WANG Z H, WANG X C, YUAN J J, et al. Survival benefit of palliative local treatments and efficacy of different pharmacotherapies in colorectal cancer with lung metastasis: results from a large retrospective study[J]. Clin Colorectal Cancer, 2018, 17(2): e233-e255. |
| [3] | 金晶, 顾晋, 沈琳. 结直肠癌肺转移多学科综合治疗专家共识(2018版)[J]. 实用肿瘤杂志, 2018, 33(6): 487-501. |
| JIN J, GU J, SHEN L. Expert consensus on multidisciplinary therapy of colorectal cancer with lung metastases (2018 edition)[J]. J Pract Oncol, 2018, 33(6): 487-501. | |
| [4] | 叶欣, 范卫君, 王徽, 等. 热消融治疗原发性和转移性肺部肿瘤专家共识(2017年版)[J]. 中国肺癌杂志, 2017, 20(7): 433-445. |
| YE X, FAN W J, WANG H, et al. Expert consensus for thermal ablation of primary and metastatic lung tumors (2017 edition)[J]. Chin J Lung Cancer, 2017, 20(7): 433-445. | |
| [5] | CERVANTES A, ADAM R, ROSELLÓ S, et al. Metastatic colorectal cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up[J]. Ann Oncol, 2023, 34(1): 10-32. |
| [6] | 中华医学会肿瘤学分会, 国家卫生健康委员会医政司. 中国结直肠癌诊疗规范(2023版)[J]. 协和医学杂志, 2023, 14(4): 706-733. |
| Oncology Branch of Chinese Medical Association; Medical Administration Bureau, National Health Commission. Chinese guidelines for the diagnosis and treatment of colorectal cancer (2023 edition)[J]. Med J Peking Union Med Coll Hosp, 2023, 14(04): 706-733. | |
| [7] | DE BAÈRE T, AUPÉRIN A, DESCHAMPS F, et al. Radiofrequency ablation is a valid treatment option for lung metastases: experience in 566 patients with 1 037 metastases[J]. Ann Oncol, 2015, 26(5): 987-991. |
| [8] | SHEN C, TANNENBAUM D, HORN R, et al. Overall survival in phase 3 clinical trials and the surveillance, epidemiology, and end results database in patients with metastatic colorectal cancer, 1986-2016: a systematic review[J]. JAMA Netw Open, 2022, 5(5): e2213588. |
| [9] | ENG C, YOSHINO T, RUÍZ-GARCÍA E, et al. Colorectal cancer[J]. Lancet, 2024, 404(10449): 294-310. |
| [10] | HUANG B Y, ZHOU J J, YU Z Q, et al. Long-term observation of CT-guided radiofrequency ablation of lung neoplasm in 476 consecutive patients by a thoracic surgical service: a single-institutional experience[J]. Acad Radiol, 2017, 24(12): 1517-1525. |
| [11] | KONG Y Q, HUANG X Y, PENG G, et al. Efficacy of first-line radiofrequency ablation combined with systemic chemotherapy plus targeted therapy for initially unresectable colorectal liver metastases[J]. Int J Hyperthermia, 2025, 42(1): 2432988. |
| [12] | LIU Y T, FAN B Q, HE J F, et al. The preliminary multicenter retrospective study on the efficacy and safety of thermal ablation for follicular thyroid neoplasms ≤3 cm[J]. Discov Oncol, 2025, 16(1): 219. |
| [13] |
NAJAFI A, DE BAERE T, PURENNE E, et al. Risk factors for local tumor progression after RFA of pulmonary metastases: a matched case-control study[J]. Eur Radiol, 2021, 31(7): 5361-5369.
doi: 10.1007/s00330-020-07675-y pmid: 33474569 |
| [14] | KURILOVA I, BENDET A, PETRE E N, et al. Factors associated with local tumor control and complications after thermal ablation of colorectal cancer liver metastases: a 15-year retrospective cohort study[J]. Clin Colorectal Cancer, 2021, 20(2): e82-e95. |
| [15] |
YANG Q X, QI H, ZHANG R, et al. Risk factors for local progression after percutaneous radiofrequency ablation of lung tumors: evaluation based on a review of 147 tumors[J]. J Vasc Interv Radiol, 2017, 28(4): 481-489.
doi: S1051-0443(16)30842-9 pmid: 28111196 |
| [16] | HUANG H Z, CHEN H, ZHENG D Z, et al. Habitat-based radiomics analysis for evaluating immediate response in colorectal cancer lung metastases treated by radiofrequency ablation[J]. Cancer Imaging, 2024, 24(1): 44. |
| [17] | HASEGAWA T, TAKAKI H, KODAMA H, et al. Impact of the ablative margin on local tumor progression after radiofrequency ablation for lung metastases from colorectal carcinoma: supplementary analysis of a phase Ⅱ trial (MLCSG-0802)[J]. J Vasc Interv Radiol, 2023, 34(1): 31-37.e1. |
| [18] | PEREIRA P L, SIEMOU P, REMPP H J, et al. CT versus MR guidance for radiofrequency ablation in patients with colorectal liver metastases: a 10-year follow-up favors MR guidance[J]. Eur Radiol, 2024, 34(7): 4663-4671. |
| [19] | SARIOGLU A G, WEHRLE C J, AKGUN E, et al. Radiofrequency ablation versus microwave ablation for colorectal liver metastases: long-term results of a retrospective cohort surgical experience[J]. Hepatobiliary Surg Nutr, 2024, 13(5): 759-770. |
| [20] |
DAVINI F, RICCIARDI S, ZIRAFA C C, et al. Lung metastasectomy after colorectal cancer: prognostic impact of resection margin on long term survival, a retrospective cohort study[J]. Int J Colorectal Dis, 2020, 35(1): 9-18.
doi: 10.1007/s00384-019-03386-z pmid: 31686201 |
| [21] | MILOSEVIC M, EDWARDS J, TSANG D, et al. Pulmonary metastasectomy in colorectal cancer: updated analysis of 93 randomized patients - control survival is much better than previously assumed[J]. Colorectal Dis, 2020, 22(10): 1314-1324. |
| [22] | TAKAYAMA T, HASEGAWA K, IZUMI N, et al. Surgery versus radiofrequency ablation for small hepatocellular carcinoma: a randomized controlled trial (SURF trial)[J]. Liver Cancer, 2021, 11(3): 209-218. |
| [23] | VAN DER LEI S, PUIJK R S, DIJKSTRA M, et al. Thermal ablation versus surgical resection of small-size colorectal liver metastases (COLLISION): an international, randomised, controlled, phase 3 non-inferiority trial[J]. Lancet Oncol, 2025, 26(2): 187-199. |
| [24] | MA Z Y, YANG S P, YANG Y L, et al. Development and validation of prediction models for the prognosis of colon cancer with lung metastases: a population-based cohort study[J]. Front Endocrinol (Lausanne), 2023, 14: 1073360. |
| [25] | LOU P W, LUO D M, HUANG Y T, et al. Establishment and validation of a prognostic nomogram for predicting postoperative overall survival in advanced stage Ⅲ-Ⅳ colorectal cancer patients[J]. Cancer Med, 2024, 13(22): e70385. |
| [26] | ZHANG S, FAN S L, WANG Z L, et al. Capecitabine regulates HSP90AB1 expression and induces apoptosis via Akt/SMARCC1/AP-1/ROS axis in T cells[J]. Oxid Med Cell Longev, 2022, 2022: 1012509. |
| [27] | GARLAND J, HUSSAIN S, RAI R, et al. Targeting HSP70-E7 interaction with SHetA2: a novel therapeutic strategy for cervical cancer[J]. J Med Virol, 2024, 96(11): e70088. |
| [28] | YOSHIMURA K, ZOU G Y, FAN Y B, et al. HSP90 inhibitor AUY922 suppresses tumor growth and modulates immune response through YAP1-TEAD pathway inhibition in gastric cancer[J]. Cancer Lett, 2025, 610: 217354. |
| [29] | SHIOZAWA M, SUNAKAWA Y, WATANABE T, et al. Modified FOLFOXIRI plus cetuximab versus bevacizumab in RAS wild-type metastatic colorectal cancer: a randomized phase Ⅱ DEEPER trial[J]. Nat Commun, 2024, 15(1): 10217. |
| [30] |
BOND M J G, BOLHUIS K, LOOSVELD O J L, et al. First-line systemic treatment for initially unresectable colorectal liver metastases: post hoc analysis of the CAIRO5 randomized clinical trial[J]. JAMA Oncol, 2025, 11(1): 36-45.
doi: 10.1001/jamaoncol.2024.5174 pmid: 39570583 |
| [31] | THIBAUDIN M, ROUSSOT N, BURLOT C, et al. Safety and efficacy of trifluridine/tipiracil +/- bevacizumab plus XB2001 (anti-IL-1α antibody): a single-center phase 1 trial[J]. Signal Transduct Target Ther, 2025, 10(1): 22. |
| [32] | HAN Y, YAN X, ZHI W H, et al. Long-term outcome following microwave ablation of lung metastases from colorectal cancer[J]. Front Oncol, 2022, 12: 943715. |
| [33] |
TAN C, FISHER O M, HUANG L N, et al. Comparison of microwave and radiofrequency ablation in the treatment of pulmonary metastasis of colorectal cancer[J]. Anticancer Res, 2022, 42(9): 4563-4571.
doi: 10.21873/anticanres.15959 pmid: 36039430 |
| [34] | ANDRÉ T, SHIU K K, KIM T W, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer[J]. N Engl J Med, 2020, 383(23): 2207-2218. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd