欢迎访问《中国癌症杂志》官方网站,今天是
分享:
中国癌症杂志 ›› 2024, Vol. 34 ›› Issue (3): 316-333.doi: 10.19401/j.cnki.1007-3639.2024.03.010
• 指南与共识 • 上一篇
中国抗癌协会乳腺癌专业委员会
收稿日期:2024-01-11
修回日期:2024-02-22
出版日期:2024-03-30
发布日期:2024-04-10
Committee of Breast Cancer Society, China Anti-Cancer Association
Received:2024-01-11
Revised:2024-02-22
Published:2024-03-30
Online:2024-04-10
文章分享
摘要:
中国乳腺癌患者发病年龄较轻,60%的女性患者在诊断时为绝经前。与绝经后相比,未绝经女性卵巢功能旺盛,可持续大量分泌雌激素、促进乳腺癌细胞增殖。卵巢功能抑制(ovarian function suppression,OFS)已用于乳腺癌临床治疗数十年,大量循证证据表明,单用OFS和加用OFS均可降低未绝经女性乳腺癌的复发风险并改善生存。部分OFS研究的长期随访数据(SOFT/TEXT研究12和13年随访、STO-5研究20年随访、亚裔人群的ASTRRA研究8年随访)近期陆续公布,进一步证实对于早期乳腺癌患者加用OFS可显著降低10年以上的复发风险,提高治愈可能。monarchE和NATALEE研究显示,部分CDK4/6抑制剂叠加在绝经前早期乳腺癌患者含有药物去势[促性腺激素释放激素类似物(gonadotropin releasing hormone analog,GnRHa)]的辅助内分泌治疗方案时仍可进一步增加生存获益。中国抗癌协会乳腺癌专业委员会召集了国内乳腺癌治疗领域的临床专家,在2021年版的基础上共同商讨编制了《中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)》。本共识建议,GnRHa仍作为绝经前激素受体阳性早期乳腺癌OFS方式的首选。GnRHa联合内分泌治疗基础上添加特定CDK4/6抑制剂的激素受体阳性绝经前乳腺癌获益人群包括:淋巴结阳性,淋巴结阴性且满足任一条件[G3,G2伴Ki-67增殖指数≥20%,G2伴多基因检测(21基因评分、Prosigna PAM50、MammaPrint、EndoPredict)高危]。本共识也认可将2023年St.Gallen共识中有化疗指征的风险因素作为OFS适用判定标准之一。GnRHa用药推荐根据激素受体阳性乳腺癌患者化疗前的卵巢功能状态进行决策。如果考虑卵巢保护,推荐GnRHa同步化疗,不影响患者生存获益;如果不考虑卵巢保护,GnRHa同步化疗和GnRHa在化疗结束后序贯使用均被认可,后者更为推荐。围绝经期患者的内分泌治疗建议参照绝经前方案。GnRHa辅助内分泌治疗的时长建议为5年。中高危患者完成5年联合GnRHa的内分泌治疗后,如果未绝经且耐受性良好,可考虑继续2~5年联合GnRHa的内分泌治疗或单用2~5年选择性雌激素受体调节剂(selective estrogen receptor modulator,SERM)治疗。辅助治疗方案中添加GnRHa安全可耐受,推荐应用前和患者充分沟通药物的使用方法和可能的不良事件,安全性管理有助于提高患者的依从性。对于接受药物去势的患者,在去势过程中不推荐常规监测雌激素水平,如怀疑不完全的OFS(包括改变用法如注射人员缺乏该药物熟练注射经验、更换剂型或出现某些可能提示卵巢功能恢复的生理变化如月经恢复或更年期症状的周期性波动时),可进行雌激素水平测定以辅助决策。绝经前乳腺癌患者如有需求,无论激素受体阳性或阴性,均可使用GnRHa保护卵巢功能,降低卵巢功能早衰的发生风险,减少生育能力损害,推荐化疗前至少1周开始使用GnRHa,每28 d 1次,直至化疗结束后2周给予最后1剂。针对激素受体阳性乳腺癌患者开展的临床试验,不推荐仅纳入绝经后人群,也应当探索GnRHa应用条件下的绝经前人群,以明确试验药物对这类患者的实际效应。另外本共识还新增了早期/局部晚期乳腺癌患者OFS药物应用的全程管理路径,以期进一步助力临床决策。
中图分类号:
中国抗癌协会乳腺癌专业委员会. 中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)[J]. 中国癌症杂志, 2024, 34(3): 316-333.
Committee of Breast Cancer Society, China Anti-Cancer Association. Expert consensus on clinical applications of ovarian function suppression for Chinese women with early breast cancer (2024 edition)[J]. China Oncology, 2024, 34(3): 316-333.
表1
绝经状态的判定标准"
| 满足以下任何一项,可判定为绝经 |
|---|
| ⑴ 既往接受过双侧卵巢切除术(或有效放疗去势) |
| ⑵ 年龄≥60岁 |
| ⑶ 年龄<60岁,自然停经≥12个月,在近1年未接受化疗、TAM、托瑞米芬或卵巢去势的情况下,FSH和E2水平在绝经后范围内 |
| ⑷ 年龄<60岁,正在服用TAM或托瑞米芬,FSH和E2水平连续两次在绝经后范围内 |
表2
经治的乳腺癌患者绝经状态的判定标准"
| 子宫完整患者的判定标准 | 对于因各种原因导致子宫不完整或子宫切除患者的判定标准 |
|---|---|
| ⑴ 年龄≥50岁,化疗后或在服用SERM药物期间闭经至少12个月,且E2及FSH水平连续测定至少3次均达到绝经后水平 | ⑴ 年龄≥50岁,化疗后满1年,且1年内至少连续3次测定E2及FSH水平均达到绝经后水平 |
| ⑵ 年龄在45~50岁,化疗后或在服用SERM药物期间闭经至少24个月,且E2及FSH水平连续测定至少3次均达到绝经后水平 | ⑵ 年龄在45~50岁,化疗后满2年,且2年内测定E2及FSH水平至少连续3次均达到绝经后水平 |
| ⑶ 年龄<45岁,由于卵巢功能恢复的概率较大,原则上不适用本标准 | ⑶ 年龄<45岁,由于卵巢功能恢复的概率较大,原则上不适用本标准 |
| ⑷ 上述标准中,年龄可参考患者家族女性平均停经年龄做出个体化调整 |
表3
绝经前激素受体阳性/HER2阴性早期乳腺癌的辅助内分泌治疗推荐临床路径"
| 危险度 | 判别要点 | 推荐方案 | |
|---|---|---|---|
| 区域淋巴结转移 | 其他危险因素 | ||
| 高危 | ≥4枚阳性 | 任何情况 | OFS+AI/TAM+阿贝西利a OFS+AI OFS+AI+瑞波西利b |
| 1~3枚阳性 | 满足以下条件之一:G3,T>5 cm,多基因检测*高危 (有化疗指征患者c推荐含OFS治疗方案) | OFS+AI/TAM+阿贝西利a OFS+AI/TAM OFS+AI+瑞波西利b | |
| 中危 | 1~3枚阳性 | 不满足高危的其他情况 (有化疗指征患者c推荐含OFS治疗方案) | OFS+AI/TAM OFS+AI+瑞波西利b |
| 阴性 | T>5 cm且侵犯皮肤胸壁或炎性乳腺癌,或2 cm<T≤5 cm且同时满足以下条件之一:G3,G2伴Ki-67增殖指数≥20%,G2伴多基因检测高危* (有化疗指征患者c推荐含OFS治疗方案) | OFS+AI/TAM OFS+AI+瑞波西利b | |
| 阴性 | 不满足低危的其他情况 (有化疗指征患者c推荐含OFS治疗方案) | OFS+AI/TAM | |
| 低危 | 阴性 | 同时满足以下条件:T≤2 cm,G1,Ki-67增殖指数<20%,无脉管癌栓,>35岁,HER2阴性 | TAM |
表4
含GnRHa辅助内分泌治疗安全管理治疗推荐"
| 相关不良事件 | 药物治疗 | 非药物治疗 |
|---|---|---|
| 血管舒缩症状:潮热,盗汗 | SSRI:帕罗西汀(不宜与SERM合用);SNRI:文拉法辛;加巴喷丁;可乐定;中医中药 | 针灸;合适的衣物 |
| 阴道症状:阴道干燥,阴道萎缩 | 阴道雌激素△:Ovestin(阴道雌三醇) | |
| 性功能障碍:性欲减退 | 非激素润滑剂,阴道保湿霜;阴道雌激素:Ovestin(阴道雌三醇) | 充分的医患沟通;放松心情 |
| 骨骼肌症状:骨质疏松,骨折 | 双膦酸盐,地舒单抗,维生素D和钙* | 负重练习;戒烟限酒;调整饮食,预防跌倒[ |
| 关节痛 | NSAID和COX-2抑制剂;维生素D | 减肥;全身抗阻力练习;物理治疗;针灸[ |
| 精神系统症状:情绪变化,如抑郁 | SSRI(如西酞普兰,依他普仑);SNRI(如文拉法辛) | 规律运动;均衡饮食;心理治疗 |
图1
早期/局部晚期乳腺癌患者OFS药物应用的全程管理路径 *:基于monarchE研究和NATALEE研究证据更新,其中瑞波西利未获批早期乳腺癌适应证,阿贝西利早期乳腺癌适应症为联合内分泌治疗(他莫昔芬或芳香化酶抑制剂)用于激素受体阳性、HER2阴性、淋巴结阳性、高复发风险的早期乳腺癌患者的辅助治疗,monarchE研究的B队列人群添加阿贝西利是否获益尚不明确;#:基于POEMS研究、PROMISE-GIM6研究、2018年J Clin Oncol的meta分析和2015年JAMA的随机对照临床试验证据更新。根据《中国抗癌协会乳腺癌诊治指南与规范(2024年版)》进行术后辅助化疗的推荐或豁免;当ER 1% ~ 10%低表达,或ER阴性/PR阳性时,考虑内分泌敏感性低,内分泌强化或延长的证据不充分;围绝经期患者应按照化疗前的激素水平、参照绝经前患者的治疗,需要联合OFS的患者,在2 ~ 5年OFS+内分泌治疗期间,如果明确判断达到了绝经状态,则方案转化为AI;患者存在BRCA1/2胚系突变情况治疗请参考OlympiA研究 [72],此处不再详细展开;STEPP复发风险评分工具:评分大于1.42分的患者为复发中高危风险人群,中高危风险人群选择5年OFS联合AI的获益优于OFS联合TAM或TAM单药。"
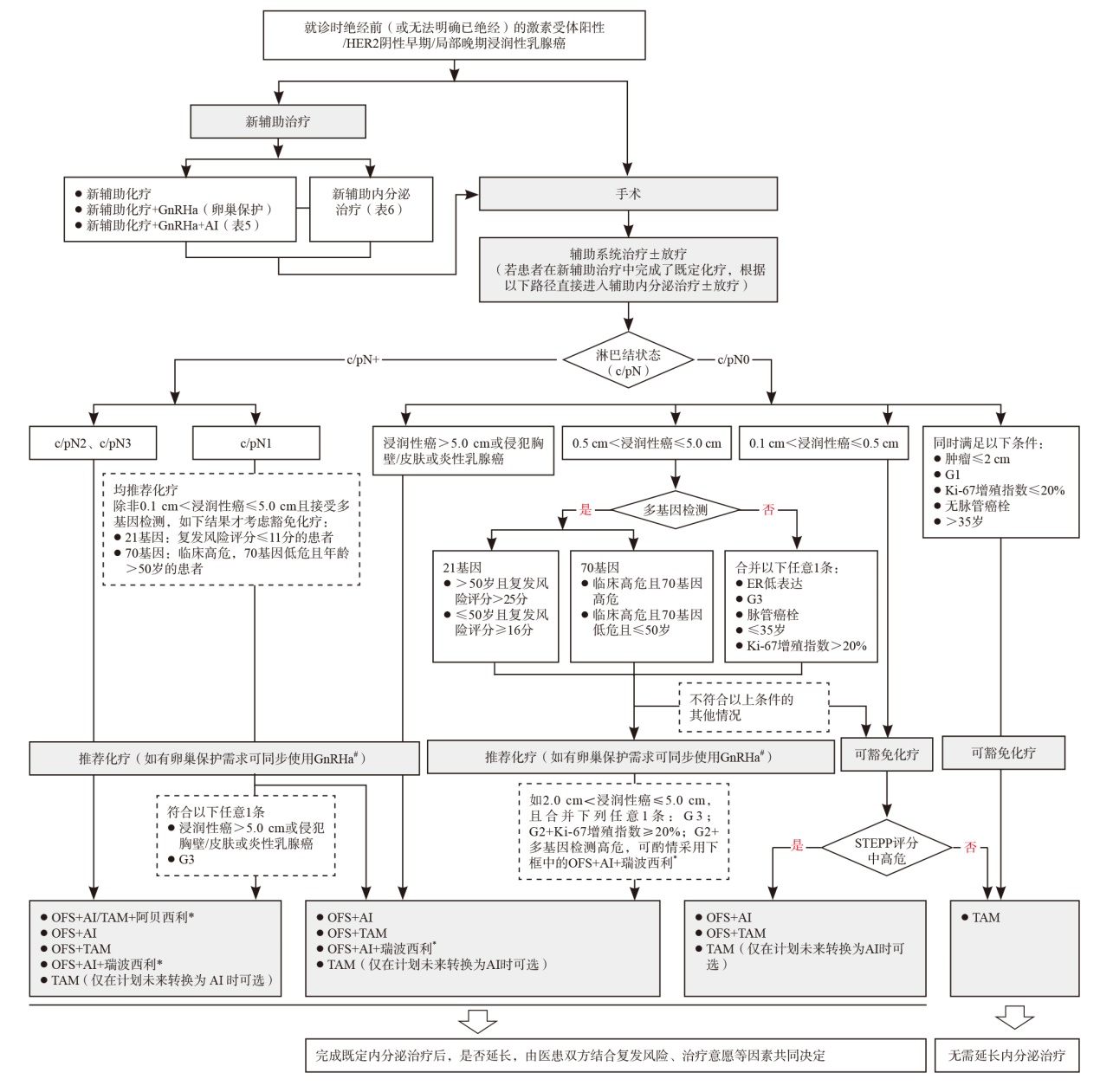
表5
绝经前激素受体阳性乳腺癌新辅助化疗联合OFS研究汇总"
| 研究名称 | 入组标准 | 样本量 | 治疗方案 | 疗效 |
|---|---|---|---|---|
| CBCSG-036[ | ⅡB ~ ⅢC期,ER阳性/HER2阴性,既往未接受过化疗和内分泌治疗,ECOG PS评分0 ~ 2分,有可测量和可评估的肿瘤原发灶,病理确诊为浸润性导管癌、年龄18 ~ 70岁、单侧乳腺癌 | 249例 | 化疗+来曲唑±OFS | 相比于单纯化疗,在新辅助化疗基础上联合雌激素剥夺治疗ER阳性/HER2阴性乳腺癌患者疗效更佳,尤其是Ki-67增殖指数较高的患者,可取得显著更高的ORR |
表6
绝经前激素受体阳性乳腺癌新辅助内分泌治疗部分研究汇总"
| 研究名称 | 入组标准 | 样本量 | 治疗方案 | 疗效 |
|---|---|---|---|---|
| STAGE[ | 绝经前激素受体阳性乳腺癌患者 | 204例 | 阿那曲唑 vs TAM | 与TAM相比,阿那曲唑组从基线至第24周的Ki-67增殖指数下降程度明显更大,其结果也显示,阿那曲唑组ORR显著优于TAM |
| IMPACT[ | 激素受体阳性乳腺癌 | 330例 | 阿那曲唑、TAM或两药联合 | 阿那曲唑、TAM和两药联合组ORR分别为37%、36%和39%,差异无统计学意义 |
| NCT02535221[ | 激素受体阳性/HER2阴性和淋巴结阴性绝经前乳腺癌患者 | 68例 | 戈舍瑞林+TAM序贯戈舍瑞林+阿那曲唑 vs 化疗 | 新辅助化疗和新辅助内分泌治疗治疗的临床缓解率分别为16.1%和35.1%,差异有统计学意义;新辅助化疗组和新辅助内分泌治疗组的保乳手术率差异无统计学意义 |
| ADAPT/ADAPTcycle[ | 临床中高危激素受体阳性/HER2阴性早期乳腺癌 | ADAPT 3 666例,ADAPT cycle 2 272例 | AI/TAM±OFS | 绝经前患者进行Ki-67增殖指数判定后的首次前瞻性数据,与大型辅助研究相比:在TAM或AI中添加OFS能够显著提高绝经前患者的内分泌治疗应答率[内分泌应答:术前2 ~ 4周短期内分泌治疗(OFS>2周)后Ki-67增殖指数≤10%],与Al治疗的绝经后患者相当 |
| ADAPTcycle[ | 临床中高危激素受体阳性/HER2阴性早期乳腺癌 | 4 334例 | TAM/AI+OFS vs TAM/AI | TAM或AI联合OFS可显著提高绝经前患者内分泌治疗反应的可能性,其发生率与AI治疗的绝经后患者相当 |
| [1] | World Health Organization. Global cancer burden growing, amidst mounting need for services[EB/OL]. (2024-02-01)[2024-02-25]. https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing-amidst-mounting-need-for-services. |
| [2] | FAN L, STRASSER-WEIPPL K, LI J J, et al. Breast cancer in China[J]. Lancet Oncol, 2014, 15(7): e279-e289. |
| [3] |
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials[J]. Lancet, 2005, 365(9472): 1687-1717.
doi: 10.1016/S0140-6736(05)66544-0 pmid: 15894097 |
| [4] |
DAVIES C, PAN H C, GODWIN J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial[J]. Lancet, 2013, 381(9869): 805-816.
pmid: 23219286 |
| [5] | GRAY R G, REA D, HANDLEY K, et al. aTTom: long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6 953 women with early breast cancer[J]. J Clin Oncol, 2013, 31(18_suppl): 5. |
| [6] |
Lhrh-Agonists in Early Breast Cancer Overview Group, CUZICK J, AMBROISINE L, et al. Use of luteinising-hormone-releasing hormone agonists as adjuvant treatment in premenopausal patients with hormone-receptor-positive breast cancer: a meta-analysis of individual patient data from randomised adjuvant trials[J]. Lancet, 2007, 369(9574): 1711-1723.
doi: 10.1016/S0140-6736(07)60778-8 pmid: 17512856 |
| [7] |
BAUM M, BUDZAR A U, CUZICK J, et al. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial[J]. Lancet, 2002, 359(9324): 2131-2139.
doi: 10.1016/s0140-6736(02)09088-8 pmid: 12090977 |
| [8] |
FRANCIS P A, PAGANI O, FLEMING G F, et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer[J]. N Engl J Med, 2018, 379(2): 122-137.
doi: 10.1056/NEJMoa1803164 |
| [9] | NOH W C, LEE J W, NAM S J, et al. Role of adding ovarian function suppression to tamoxifen in young women with hormone-sensitive breast cancer who remain premenopausal or resume menstruation after chemotherapy: the ASTRRA study[J]. J Clin Oncol, 2018, 36(15_suppl): 502. |
| [10] | PERRONE F, DE LAURENTIIS M, DE PLACIDO S, et al. The HOBOE-2 multicenter randomized phase Ⅲ trial in premenopausal patients with hormone-receptor positive early breast cancer comparing triptorelin plus either tamoxifen or letrozole or letrozole + zoledronic acid[J]. Ann Oncol, 2018, 29: Ⅷ704. |
| [11] | REGAN M M, WALLEY B A, FLEMING G F, et al. Abstract GS2-05: randomized comparison of adjuvant aromatase inhibitor exemestane (E) plus ovarian function suppression (OFS) vs tamoxifen (T) plus OFS in premenopausal women with hormone receptor-positive (HR+) early breast cancer (BC): update of the combined TEXT and SOFT trials[J]. Cancer Res, 2022, 82(4_Supplement): GS2-5-GS2-05. |
| [12] | FRANCIS P A, FLEMING G F, LÁNG I, et al. Adjuvant endocrine therapy in premenopausal breast cancer: 12-year results from SOFT[J]. J Clin Oncol, 2023, 41(7): 1370-1375. |
| [13] | JOHANSSON A, DAR H, VAN’T VEER L J, et al. Twenty-year benefit from adjuvant goserelin and tamoxifen in premenopausal patients with breast cancer in a controlled randomized clinical trial[J]. J Clin Oncol, 2022, 40(35): 4071-4082. |
| [14] |
JOHNSTON S R D, HARBECK N, HEGG R, et al. Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2-, node-positive, high-risk, early breast cancer (monarchE)[J]. J Clin Oncol, 2020, 38(34): 3987-3998.
doi: 10.1200/JCO.20.02514 |
| [15] |
JOHNSTON S R D, TOI M, O’SHAUGHNESSY J, et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial[J]. Lancet Oncol, 2023, 24(1): 77-90.
doi: 10.1016/S1470-2045(22)00694-5 |
| [16] | BARDIA A, HORTOBAGYI G, LIPATOV O, et al. Invasive disease-free survival across key subgroups from the phase Ⅲ NATALEE study of ribociclib + a nonsteroidalaromatase inhibitor in patients with HR+/HER2- early breast cancer[J]. Ann Oncol, 2023, 34(suppl2): S1261-S1262. |
| [17] | SLAMON D J, STROYAKOVSKIY D, YARDLEY D A, et al. Ribociclib and endocrine therapy as adjuvant treatment in patients with HR+/HER2- early breast cancer: primary results from the phase Ⅲ NATALEE trial[J]. J Clin Oncol, 2023, 41(17_suppl): LBA500. |
| [18] |
SLAMON D, LIPATOV O, NOWECKI Z, et al. Ribociclib plus endocrine therapy in early breast cancer[J]. N Engl J Med, 2024, 390(12): 1080-1091.
doi: 10.1056/NEJMoa2305488 |
| [19] |
WANG X, XIA C F, WANG Y, et al. Landscape of young breast cancer under 35 years in China over the past decades: a multicentre retrospective cohort study (YBCC-Catts study)[J]. EClinicalMedicine, 2023, 64: 102243.
doi: 10.1016/j.eclinm.2023.102243 |
| [20] |
中国抗癌协会乳腺癌专业委员会, 中华医学会肿瘤学分会乳腺肿瘤学组. 中国抗癌协会乳腺癌诊治指南与规范(2024年版)[J]. 中国癌症杂志, 2023, 33(12): 1092-1187.
doi: 10.19401/j.cnki.1007-3639.2023.12.004 |
| The Society of Breast Cancer China Anti-Cancer Association, Breast Oncology Group of the Oncology Branch of the Chinese Medical Association. Guidelines for breast cancer diagnosis and treatment by China Anti-Cancer Association (2024 edition)[J]. China Oncol, 2023, 33(12): 1092-1187. | |
| [21] |
HARRISON G S, WIERMAN M E, NETT T M, et al. Gonadotropin-releasing hormone and its receptor in normal and malignant cells[J]. Endocr Relat Cancer, 2004, 11(4): 725-748.
doi: 10.1677/erc.1.00777 |
| [22] | DOISNEAU-SIXOU S F, SERGIO C M, CARROLL J S, et al. Estrogen and antiestrogen regulation of cell cycle progression in breast cancer cells[J]. Endocr Relat Cancer, 2003, 10(2): 179-186. |
| [23] |
TAN S H, WOLFF A C. Luteinizing hormone-releasing hormone agonists in premenopausal hormone receptor-positive breast cancer[J]. Clin Breast Cancer, 2007, 7(6): 455-464.
doi: 10.3816/CBC.2007.n.002 |
| [24] |
MCDONALD WADE S 3RD, HACKNEY M H, KHATCHERESSIAN J, et al. Ovarian suppression in the management of premenopausal breast cancer: methods and efficacy in adjuvant and metastatic settings[J]. Oncology, 2008, 75(3/4): 192-202.
doi: 10.1159/000163059 |
| [25] | National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guideline®). Breast Cancer, version 5. 2023[EB/OL]. [2024-01-12]. https://www.nccn.org/guidelines/guidelines-detail?category=1&id =1419. |
| [26] | 中国临床肿瘤学会指南工作委员会. 中国临床肿瘤学会(CSCO)乳腺癌诊疗指南(2023)[M]. 北京: 人民卫生出版社, 2023. |
| Chinese Society of Clinical Oncology Guidelines Working Committee. Guidelines of Chinese Society of Clinical Oncology on breast cancer (2023)[M]. Beijing: People’s Medical Publishing House, 2023. | |
| [27] |
PINTO MARÍN A, BALLESTEROS GARCÍA A I, IZARZUGAZA PERÓN Y, et al. Adjuvant hormonal therapy in perimenopausal patients[J]. Adv Ther, 2011, 28(Suppl 6): 39-49.
doi: 10.1007/s12325-011-0023-3 |
| [28] |
FRANCIS P A, REGAN M M, FLEMING G F, et al. Adjuvant ovarian suppression in premenopausal breast cancer[J]. N Engl J Med, 2015, 372(5): 436-446.
doi: 10.1056/NEJMoa1412379 |
| [29] | 中国抗癌协会乳腺癌专业委员会. 中国绝经前女性乳腺癌患者辅助治疗后绝经判断标准及芳香化酶临床应用共识(草案修正案)[J]. 中国癌症杂志, 2011, 21(5): 418-420. |
| The Society of Breast Cancer China Anti-Cancer Association. Postmenopausal criteria for menopausal women and clinical consensus on aromatase application in China’s pre-menopausal women with breast cancer (draft amendment)[J]. China Oncol, 2011, 21(5): 418-420. | |
| [30] | 乐杰. 妇产科学复习考试指南[M]. 2版. 北京: 人民卫生出版社, 2000. |
| LE J. Guidelines for obstetrics and gynecology review examination[M]. 2nd edition. Beijing: People’s Medical Publishing House, 2000. | |
| [31] |
DEES E C, DAVIDSON N E. Ovarian ablation as adjuvant therapy for breast cancer[J]. Semin Oncol, 2001, 28(4): 322-331.
pmid: 11498826 |
| [32] |
JONAT W, KAUFMANN M, SAUERBREI W, et al. Goserelin versus cyclophosphamide, methotrexate, and fluorouracil as adjuvant therapy in premenopausal patients with node-positive breast cancer: the Zoladex Early Breast Cancer Research Association study[J]. J Clin Oncol, 2002, 20(24): 4628-4635.
pmid: 12488406 |
| [33] | BUI K T, WILLSON M L, GOEL S, et al. Ovarian suppression for adjuvant treatment of hormone receptor-positive early breast cancer[J]. Cochrane Database Syst Rev, 2020, 3(3): CD013538. |
| [34] |
BURSTEIN H J, LACCHETTI C, ANDERSON H, et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American Society of Clinical Oncology clinical practice guideline update on ovarian suppression[J]. J Clin Oncol, 2016, 34(14): 1689-1701.
doi: 10.1200/JCO.2015.65.9573 pmid: 26884586 |
| [35] |
BAEK S Y, NOH W C, AHN S H, et al. Adding ovarian function suppression to tamoxifen in young women with hormone-sensitive breast cancer who remain premenopausal or resume menstruation after chemotherapy: 8-year follow-up of the randomized ASTRRA trial[J]. J Clin Oncol, 2023, 41(31): 4864-4871.
doi: 10.1200/JCO.23.00557 |
| [36] |
THOMSSEN C, BALIC M, HARBECK N, et al. St. Gallen/Vienna 2021: a brief summary of the consensus discussion on customizing therapies for women with early breast cancer[J]. Breast Care, 2021, 16(2): 135-143.
doi: 10.1159/000516114 pmid: 34002112 |
| [37] |
PALUCH-SHIMON S, CARDOSO F, PARTRIDGE A H, et al. ESO-ESMO fifth international consensus guidelines for breast cancer in young women (BCY5)[J]. Ann Oncol, 2022, 33(11): 1097-1118.
doi: 10.1016/j.annonc.2022.07.007 |
| [38] |
LAN B, MA F, ZHAI X, et al. The relationship between the CYP2D6 polymorphisms and tamoxifen efficacy in adjuvant endocrine therapy of breast cancer patients in Chinese Han population[J]. Int J Cancer, 2018, 143(1), 184-189.
doi: 10.1002/ijc.31291 pmid: 29396856 |
| [39] |
ALLISON K H, HAMMOND M E H, DOWSETT M, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update[J]. J Clin Oncol, 2020, 38(12): 1346-1366.
doi: 10.1200/JCO.19.02309 pmid: 31928404 |
| [40] |
CURIGLIANO G, BURSTEIN H J, GNANT M, et al. Understanding breast cancer complexity to improve patient outcomes: the St. Gallen international consensus conference for the primary therapy of individuals with early breast cancer 2023[J]. Ann Oncol, 2023, 34(11): 970-986.
doi: 10.1016/j.annonc.2023.08.017 pmid: 37683978 |
| [41] |
PAGANI O, REGAN M M, WALLEY B A, et al. Adjuvant exemestane with ovarian suppression in premenopausal breast cancer[J]. N Engl J Med, 2014, 371(2): 107-118.
doi: 10.1056/NEJMoa1404037 |
| [42] |
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials[J]. Lancet, 2015, 386(10001): 1341-1352.
doi: S0140-6736(15)61074-1 pmid: 26211827 |
| [43] | REGAN M M, FRANCIS P A, PAGANI O, et al. Absolute improvements in freedom from distant recurrence with adjuvant endocrine therapy for premenopausal women with HR+ HER2- negative breast cancer: results from TEXT and SOFT[J]. J Clin Oncol, 2018, 36(suppl 15): 503-503. |
| [44] | PERRONE F, LAURENTIIS M D, PLACIDO S D, et al. The HOBOE-2 multicenter randomized phase 3 trial in premenopausal patients with hormone-receptor positive early breast cancer comparing triptorelin plus either tamoxifen or letrozole or letrozole + zoledronic acid[J]. Ann Oncol, 2018, 29(suppl 8). [Epub ahead of print] |
| [45] |
LAMBERTINI M, BONI, MICHELOTTI A, et al. Ovarian suppression with triptorelin during adjuvant breast cancer chemotherapy and long-term ovarian function, pregnancies, and disease-free survival: a randomized clinical trial[J]. JAMA, 2015, 314(24): 2632-2640.
doi: 10.1001/jama.2015.17291 pmid: 26720025 |
| [46] |
LAMBERTINI M, MOORE H C F, LEONARD R C F, et al. Gonadotropin-releasing hormone agonists during chemotherapy for preservation of ovarian function and fertility in premenopausal patients with early breast cancer: a systematic review and meta-analysis of individual patient-level data[J]. J Clin Oncol, 2018, 36(19): 1981-1990.
doi: 10.1200/JCO.2018.78.0858 pmid: 29718793 |
| [47] |
HACKSHAW A, BAUM M, FORNANDER T, et al. Long-term effectiveness of adjuvant goserelin in premenopausal women with early breast cancer[J]. J Natl Cancer Inst, 2009, 101(5): 341-349.
doi: 10.1093/jnci/djn498 pmid: 19244174 |
| [48] |
GNANT M, MLINERITSCH B, STOEGER H, et al. Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 62-month follow-up from the ABCSG-12 randomised trial[J]. Lancet Oncol, 2011, 12(7): 631-641.
doi: 10.1016/S1470-2045(11)70122-X pmid: 21641868 |
| [49] | GNANT M, DUECK A C, FRANTAL S, et al. Adjuvant palbociclib for early breast cancer: the PALLAS trial results (ABCSG-42/AFT-05/BIG-14-03)[J]. J Clin Oncol, 2022, 40(3): 282-293. |
| [50] | FURLANETTO J, MARMÉ F, THODE C, et al. Ovarian function in young patients (pts) treated with postneoadjuvant palbociclib (PAL) and endocrine therapy (ET) for hormone receptor (HR)-positive, HER2-negative early breast cancer (BC): explorative analysis in PENELOPE-B[J]. Ann Oncol, 2022, 33(suppl_3): S148-S164. |
| [51] |
PAN H C, GRAY R, BRAYBROOKE J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years[J]. N Engl J Med, 2017, 377(19): 1836-1846.
doi: 10.1056/NEJMoa1701830 |
| [52] | 葛睿, 王碧芸, 江泽飞, 等. 乳腺癌CDK4/6抑制剂相关性不良反应管理共识[J]. 中华肿瘤杂志, 2022, 44(12): 1296-1304. |
| GE R, WANG B Y, JIANG Z F, et al. Expert consensus on the management of adverse events of CDK4/6 inhibitors in breast cancer[J]. Chin J Oncol, 2022, 44(12): 1296-1304. | |
| [53] |
HICKEY M, SAUNDERS C, PARTRIDGE A, et al. Practical clinical guidelines for assessing and managing menopausal symptoms after breast cancer[J]. Ann Oncol, 2008, 19(10): 1669-1680.
doi: 10.1093/annonc/mdn353 pmid: 18522932 |
| [54] |
MOORE H C, UNGER J M, PHILLIPS K A, et al. Goserelin for ovarian protection during breast-cancer adjuvant chemotherapy[J]. N Engl J Med, 2015, 372(10): 923-932.
doi: 10.1056/NEJMoa1413204 |
| [55] | 陈璐, 刘均娥, 赵福云, 等. 乳腺癌患者骨安全管理的证据总结[J]. 中国护理管理, 2022, 22(12): 1844-1848. |
| CHEN L, LIU J E, ZHAO F Y, et al. Bone safety management in breast cancer survivors: an evidence summary[J]. Chin Nurs Manag, 2022, 22(12): 1844-1848. | |
| [56] |
PETREK J A, NAUGHTON M J, CASE L D, et al. Incidence, time course, and determinants of menstrual bleeding after breast cancer treatment: a prospective study[J]. J Clin Oncol, 2006, 24(7): 1045-1051.
doi: 10.1200/JCO.2005.03.3969 pmid: 16476708 |
| [57] | LIEM G S, MO F K, PANG E, et al. Chemotherapy-related amenorrhea and menopause in young Chinese breast cancer patients: analysis on incidence, risk factors and serum hormone profiles[J]. PLoS One, 2015, 10(10): e0140842. |
| [58] |
SMITH I E, DOWSETT M, YAP Y S, et al. Adjuvant aromatase inhibitors for early breast cancer after chemotherapy-induced amenorrhoea: caution and suggested guidelines[J]. J Clin Oncol, 2006, 24(16): 2444-2447.
pmid: 16735701 |
| [59] | 宋三泰, 陈建魁, 单彬. 规范乳腺癌性激素化验报告理顺应用AIs的绝经标准[J]. 中华乳腺病杂志(电子版), 2012, 6(3): 238-243. |
| SONG S T, CHEN J K, SHAN B. Standardizing the report of sex hormone test for breast cancer and rationalizing the menopause standard of AIs[J]. Chin J Breast Dis (Electron Ed), 2012, 6(3): 238-243. | |
| [60] | 江泽飞, 王晓迪. 乳腺癌内分泌治疗十个热点问题的思考[J]. 中华外科杂志, 2015, 53(12): 895-900. |
| JIANG Z F, WANG X D. Consideration and discussion on ten hot issues of endocrine therapy for breast cancer[J]. Chin J Surg, 2015, 53(12): 895-900. | |
| [61] |
BOCCARDO F, RUBAGOTTI A, AMOROSO D, et al. Endocrinological and clinical evaluation of two depot formulations of leuprolide acetate in pre- and perimenopausal breast cancer patients[J]. Cancer Chemother Pharmacol, 1999, 43(6): 461-466.
doi: 10.1007/s002800050924 |
| [62] |
MASUDA N, IWATA H, RAI Y, et al. Monthly versus 3-monthly goserelin acetate treatment in pre-menopausal patients with estrogen receptor-positive early breast cancer[J]. Breast Cancer Res Treat, 2011, 126(2): 443-451.
doi: 10.1007/s10549-010-1332-y |
| [63] | 范蕾, YEH Yu-Chen, 杜芬, 等. 中国绝经前激素受体阳性乳腺癌辅助内分泌治疗最小成本分析[J]. 中国药物经济学, 2020, 15(4): 5-10. |
| FAN L, YEH Y C, DU F, et al. Analysis on minimum cost of adjuvant endocrine therapy in premenopausal hormone receptorpositive breast cancer in China[J]. China J Pharm Econ, 2020, 15(4): 5-10. | |
| [64] | 江泽飞, 李健斌. 新型冠状病毒肺炎疫情下乳腺癌诊疗十个热点问题的思考[J]. 中华医学杂志, 2020, 100(10): 721-723. |
| JIANG Z F, LI J B. Ten hot issues on diagnosis and treatment of breast cancer under the outbreak of novel coronavirus pneumonia[J]. Natl Med J China, 2020, 100(10): 721-723. | |
| [65] |
MOORE H C F, UNGER J M, PHILLIPS K A, et al. Final analysis of the prevention of early menopause study (POEMS)/SWOG Intergroup S0230[J]. J Natl Cancer Inst, 2019, 111(2): 210-213.
doi: 10.1093/jnci/djy185 pmid: 30371800 |
| [66] |
MICHELOTTI A, et al. Effect of the gonadotropin-releasing hormone analogue triptorelin on the occurrence of chemotherapy-induced early menopause in premenopausal women with breast cancer: a randomized trial[J]. JAMA, 2011, 306(3): 269-276.
doi: 10.1001/jama.2011.991 pmid: 21771987 |
| [67] |
LAMBERTINI M, BONI L, MICHELOTTI A, et al. Final analysis of the PROMISE-GIM6 phase Ⅲ trial assessing GnRH agonist use during chemotherapy as a strategy to preserve ovarian function in premenopausal patients with early breast cancer[J]. J Clin Oncol, 2021, 39(suppl 15): 516-516.
doi: 10.1200/JCO.2021.39.15_suppl.516 |
| [68] | CARDOSO F, KYRIAKIDES S, OHNO S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2019, 30(10): 1674. |
| [69] | 中国年轻乳腺癌诊疗与生育管理专家共识专家委员会. 年轻乳腺癌诊疗与生育管理专家共识[J]. 中华肿瘤杂志, 2019, 41(7):486-495. |
| Expert Committee on China’s Young Breast Cancer Diagnosis and Treatment and Fertility Management Expert Consensus. Expert consensus on diagnosis and treatment and birth management for young breast cancer[J]. Chin J Oncol, 2019, 41(7): 486-495. | |
| [70] | Premenopausal women with breast cancer: developing drugs for treatment guidance for industry[P]. FDA, 2020, 2020-D-1553. |
| [71] |
GAO J J, KROL D, NARAYAN P, et al. Bringing safe and effective therapies to premenopausal women with breast cancer: efforts to broaden eligibility criteria[J]. Ann Oncol, 2021, 32(8): 950-953.
doi: 10.1016/j.annonc.2021.05.356 pmid: 33991601 |
| [72] |
TUTT A N J, GARBER J E, KAUFMAN B, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer[J]. N Engl J Med, 2021, 384(25): 2394-2405.
doi: 10.1056/NEJMoa2105215 |
| [73] |
YU K D, WU S Y, LIU G Y, et al. Concurrent neoadjuvant chemotherapy and estrogen deprivation in patients with estrogen receptor-positive, human epidermal growth factor receptor 2-negative breast cancer (CBCSG-036): a randomized, controlled, multicenter trial[J]. Cancer, 2019, 125(13): 2185-2193.
doi: 10.1002/cncr.32057 |
| [74] |
MASUDA N, SAGARA Y, KINOSHITA T, et al. Neoadjuvant anastrozole versus tamoxifen in patients receiving goserelin for premenopausal breast cancer (STAGE): a double-blind, randomised phase 3 trial[J]. Lancet Oncol, 2012, 13(4): 345-352.
doi: 10.1016/S1470-2045(11)70373-4 pmid: 22265697 |
| [75] |
SMITH I E, DOWSETT M, EBBS S R, et al. Neoadjuvant treatment of postmenopausal breast cancer with anastrozole, tamoxifen, or both in combination: the immediate preoperative anastrozole, tamoxifen, or combined with tamoxifen (IMPACT) multicenter double-blind randomized trial[J]. J Clin Oncol, 2005, 23(22): 5108-5116.
doi: 10.1200/JCO.2005.04.005 pmid: 15998903 |
| [76] | GU C S, HE Y J, LI J F, et al. Efficacy of neoadjuvant endocrine therapy compared with neoadjuvant chemotherapy in pre-menopausal patients with hormone-responsive and HER2-negative, lymph node-negative breast cancer[J]. Cancer Res, 83(5_suppl): P5-09-04. |
| [77] | GLUZ O, NITZ U A, CHRISTGEN M, et al. Impact of age, recurrence score (RS) and ovarian function suppression (OFS) on endocrine response to short preoperative endocrine therapy (ET): analysis of ADAPT and ADAPTcycle trials[J]. Ann Oncol, 2022, 33: S1382-S1383. |
| [78] | OLEG G. Impact of age and ovarian function suppression (OFS) on endocrine response to short preoperative endocrine therapy (ET): results from the multicenter ADAPTcycle trial (n = 4 334)[R]. San Antonio: SABCS, 2023. |
| [1] | 王稚晴, 刘西禹, 范蕾. 早期乳腺癌辅助治疗的进展和争议[J]. 中国癌症杂志, 2025, 35(3): 255-262. |
| [2] | 王小波, 王涛. 2024年度晚期乳腺癌共识与争议的现状及展望[J]. 中国癌症杂志, 2025, 35(3): 263-272. |
| [3] | 李彬, 陶中华, 胡夕春. CDK4/6抑制剂后时代下的乳腺癌精准诊疗[J]. 中国癌症杂志, 2025, 35(3): 273-282. |
| [4] | 吴春晓, 庞怡, 顾凯, 颜佳颖, 王春芳, 向詠梅, 施燕. 2002—2017年上海市女性乳腺癌生存分析[J]. 中国癌症杂志, 2025, 35(3): 291-297. |
| [5] | 卢愚风, 王晗, 谢亦璠, 江一舟, 邵志敏. 中国乳腺癌重要基础转化研究——进展与展望[J]. 中国癌症杂志, 2025, 35(2): 143-153. |
| [6] | 林佳琳, 王文娜, 徐兵河. 抗体药物偶联物在乳腺癌领域的研究现状与展望[J]. 中国癌症杂志, 2025, 35(2): 154-166. |
| [7] | 杨鑫, 史钱枫, 刘强. 2024年中国乳腺癌重要临床研究成果[J]. 中国癌症杂志, 2025, 35(2): 167-175. |
| [8] | 黎星, 彭子琪, 于鑫淼, 金锋. 2024年改变早期乳腺癌临床实践的重要研究成果及进展[J]. 中国癌症杂志, 2025, 35(2): 176-185. |
| [9] | 吴淞, 袁洋, 江泽飞. 2024年改变晚期乳腺癌临床实践的重要研究进展[J]. 中国癌症杂志, 2025, 35(2): 186-194. |
| [10] | 曾成, 王沅怡, 王佳妮, 马飞. 乳腺癌免疫检查点抑制剂治疗的研究进展与探索方向[J]. 中国癌症杂志, 2025, 35(2): 195-204. |
| [11] | 李俊杰. 早期乳腺癌局部治疗与全身治疗的进展与展望[J]. 中国癌症杂志, 2025, 35(2): 205-212. |
| [12] | 王青, 俞育帅, 王晨曦, 姜子荣, 李佳璐, 唐诗聪, 宋传贵. 三级淋巴结构异质性在三阴性乳腺癌新辅助治疗中的预测作用及免疫微环境特征的研究现状与展望[J]. 中国癌症杂志, 2025, 35(2): 213-218. |
| [13] | 逯永晋, 石志强, 李彤, 王永胜, 邱鹏飞. 乳腺癌前哨淋巴结阳性豁免腋窝清扫后区域淋巴结放疗的回顾性研究[J]. 中国癌症杂志, 2025, 35(2): 228-236. |
| [14] | 蔡舒玥, 谢佺, 周雨萱, 刘清竹, 邱玲, 林建国. NRP-1靶向分子探针助力乳腺癌诊断的最新进展及展望[J]. 中国癌症杂志, 2025, 35(2): 249-254. |
| [15] | 徐睿, 王泽浩, 吴炅. 肿瘤相关中性粒细胞在乳腺癌发生、发展中的作用研究进展[J]. 中国癌症杂志, 2024, 34(9): 881-889. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
地址:上海市徐汇区东安路270号复旦大学附属肿瘤医院10号楼415室
邮编:200032 电话:021-64188274 E-mail:zgazzz@china-oncology.com
访问总数:; 今日访问总数:; 当前在线人数:
本系统由北京玛格泰克科技发展有限公司设计开发 技术支持:support@magtech.com.cn