欢迎访问《中国癌症杂志》官方网站,今天是
分享:
中国癌症杂志 ›› 2023, Vol. 33 ›› Issue (1): 54-60.doi: 10.19401/j.cnki.1007-3639.2023.01.006
庄晗( ), 凌池芳, 王佳舟, 韩序, 姜睿, 胡伟刚()
), 凌池芳, 王佳舟, 韩序, 姜睿, 胡伟刚()
ZHUANG Han(), LING Chifang, WANG Jiazhou, HAN Xu, JIANG Rui, HU Weigang()
摘要:
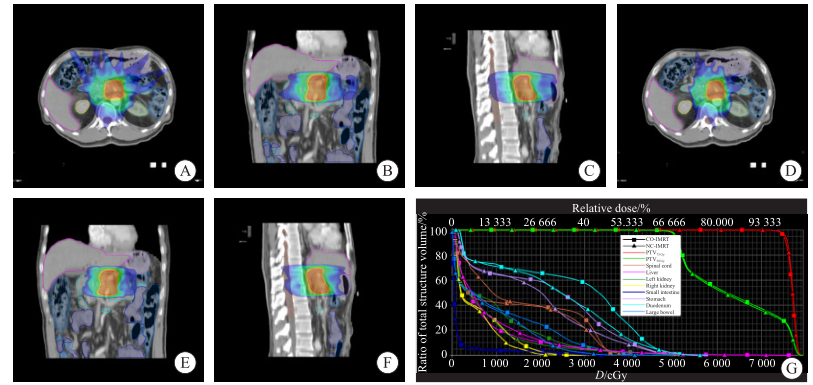
背景与目的:近年来,胰腺癌的发病率逐年上升,调强放射治疗(intensity-modulated radiotherapy,IMRT)已被广泛应用于胰腺癌的治疗,但多数胰腺癌IMRT的剂量学研究的处方剂量都小于60 Gy。本研究旨在探究局部晚期胰腺癌(locally advanced pancreatic cancer,LAPC)患者75 Gy同步加量放射治疗的剂量可行性并比较共面IMRT(coplanar IMRT,CO-IMRT)与非共面IMRT(non-coplanar IMRT,NC-IMRT)技术的剂量学差异。方法:纳入复旦大学附属肿瘤医院2018年1月—2021年12月收治的符合入组标准的10例接受同步加量放射治疗的LAPC患者,处方剂量为50 Gy的计划靶区(planning target volume,PTV),记为PTV50 Gy,处方剂量为75 Gy同步加量的PTV,记为PTV75 Gy,靶区照射分次均为25次。为每例患者分别设计CO-IMRT和NC-IMRT计划。同1例患者两种计划的射野数、处方剂量和危及器官(organs at risk,OAR)的优化条件完全相同。统计CO-IMRT和NC-IMRT计划的靶区剂量分布、适形性指数(conformity index,CI)、均匀性指数(homogeneity index,HI)、OAR剂量学结果、出束时间和机器跳数(monitor units,MU)。评估靶区是否满足临床要求以及OAR剂量限值是否符合临床正常组织效应定量分析(quantitative analysis of normal tissue effects in the clinic,QUANTEC)要求,并比较CO-IMRT计划与NC-IMRT计划之间的剂量学差异。结果:CO-IMRT和NC-IMRT均可达到靶区剂量覆盖要求并满足QUANTEC的剂量限值要求。两种PTV的CI、HI、出束时间和MU之间的差异无统计学意义(P>0.05)。在左侧肾Dmean[(10.15±1.53)Gy vs(9.29±1.78)Gy,P<0.05]、左侧肾V12[(32.74±7.45)% vs(26.03±8.97)%,P<0.05]、右侧肾Dmean[(7.37±2.41)Gy vs(6.62±2.37)Gy,P<0.05]、右侧肾V12[(22.27±10.30)% vs(14.94±8.62)%,P<0.05]、肝V30[(6.37±4.05)% vs(5.47±3.70)%,P<0.05]、小肠V30[(9.96±6.66)% vs(8.73±6.19)%,P<0.05]、小肠V45[(1.15±0.71)% vs(0.96±0.61)%,P<0.05]、胃V45[(5.37±3.96)% vs(4.52±3.32)%,P<0.05]、大肠V30[(13.18±4.95)% vs(9.19±4.94)%,P<0.05]指标上,NC-IMRT显著优于CO-IMRT,差异有统计学意义(P<0.05)。在脊髓Dmax、肝Dmean、双侧肾V20、双侧肾V28、小肠Dmax、胃Dmax和十二指肠V55(mL)指标上,CO-IMRT与NC-IMRT之间差异无统计学意义(P>0.05)。结论:基于75 Gy同步加量放射治疗治疗LAPC时,CO-IMRT和NC-IMRT均能达到靶区剂量覆盖要求并满足OAR剂量限值。在不影响靶区剂量覆盖质量的前提下,NC-IMRT在双肾、肝和胃肠道的剂量分布上更有优势,能够更好地保护OAR,降低放射治疗对胃肠道、肝和肾的毒性。
中图分类号: