欢迎访问《中国癌症杂志》官方网站,今天是
分享:
中国癌症杂志 ›› 2025, Vol. 35 ›› Issue (9): 884-892.doi: 10.19401/j.cnki.1007-3639.2025.09.009
钟佳倩( ), 李家平, 谢晓燕, 郑艳玲()
), 李家平, 谢晓燕, 郑艳玲()
收稿日期:2025-02-14
修回日期:2025-06-12
出版日期:2025-09-30
发布日期:2025-10-17
通信作者:
郑艳玲
作者简介:钟佳倩(ORCID: 0000-0002-1509-659X),硕士研究生在读。
ZHONG Jiaqian(), LI Jiaping, XIE Xiaoyan, ZHENG Yanling()
Received:2025-02-14
Revised:2025-06-12
Published:2025-09-30
Online:2025-10-17
Contact:
ZHENG Yanling
文章分享
摘要:
乳腺癌患者新辅助治疗(neoadjuvant therapy,NAT)后的腋窝管理正在优化,目前针对腋窝淋巴结(axillary lymph node,ALN)状态的评估,前哨淋巴结活检(sentinel lymph node biopsy,SLNB)已经成为重要手段,尤其是在初始临床ALN阴性(clinically negative ALN,cN0)的早期乳腺癌患者中,可以替代传统的ALN清扫(ALN dissection,ALND),减少不必要的手术风险和并发症,但是SLNB在初始临床ALN阳性(clinically positive ALN,cN+)的乳腺癌患者NAT后的应用上存在着一些假阴性率(false negative rate,FNR)及差异。通过切除≥3个SLN、使用双重示踪剂(如放射性核素联合蓝染料)或结合免疫组织化学(immunohistochemistry,IHC)进行病理学评估,可将其FNR显著降低至可接受范围(4.9%~9.1%),并且发展出多种优化方案如放射性碘粒子标记ALN(marking ALN with radioactive iodine,MARI)、靶向腋窝清扫(targeted axillary dissection,TAD)、放射性碘粒子标记联合SLNB(radioactive iodine seed placement in the axilla with SLNB,RISAS),均表现出低FNR。不仅如此,非侵入性影像技术如正电子发射计算机体层成像(positron emission tomography and computed tomography,PET/CT)、磁共振成像(magnetic resonance imaging,MRI)、常规超声及超声造影(contrast-enhanced ultrasound,CEUS)都可以用于评估NAT后的腋窝反应,其诊断效能各异。本文对近年来cN+的乳腺癌患者NAT后的腋窝管理及SLNB诊治优化的相关研究进行总结。
中图分类号:
钟佳倩, 李家平, 谢晓燕, 郑艳玲. 乳腺癌新辅助治疗后的腋窝管理及前哨淋巴结诊治的优化[J]. 中国癌症杂志, 2025, 35(9): 884-892.
ZHONG Jiaqian, LI Jiaping, XIE Xiaoyan, ZHENG Yanling. Axillary management after neoadjuvant therapy for breast cancer and optimization of sentinel lymph node diagnosis and treatment[J]. China Oncology, 2025, 35(9): 884-892.
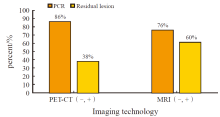
图1
代谢成像(PET/CT)与解剖成像(MRI)的互补性与局限性"
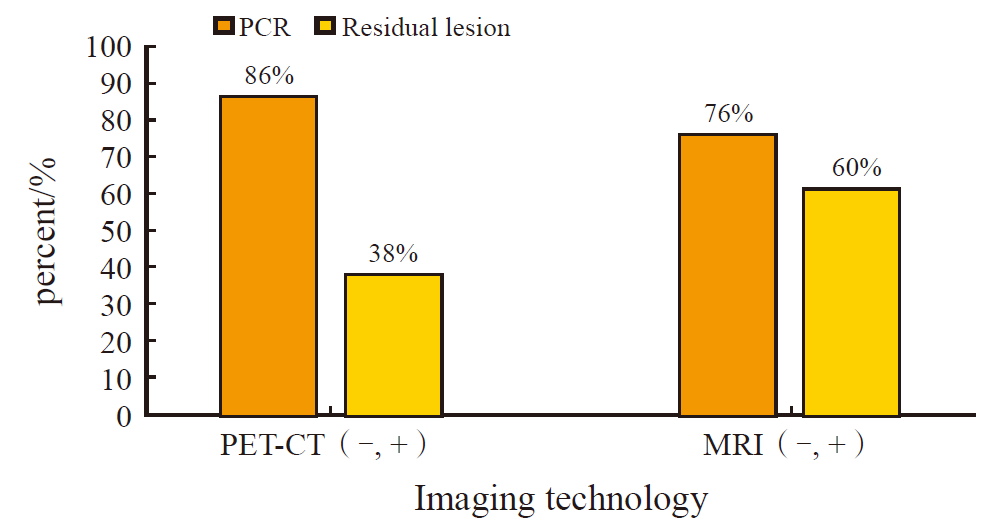
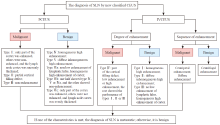
图 2
新分类CEUS联合诊断SLN的流程图"
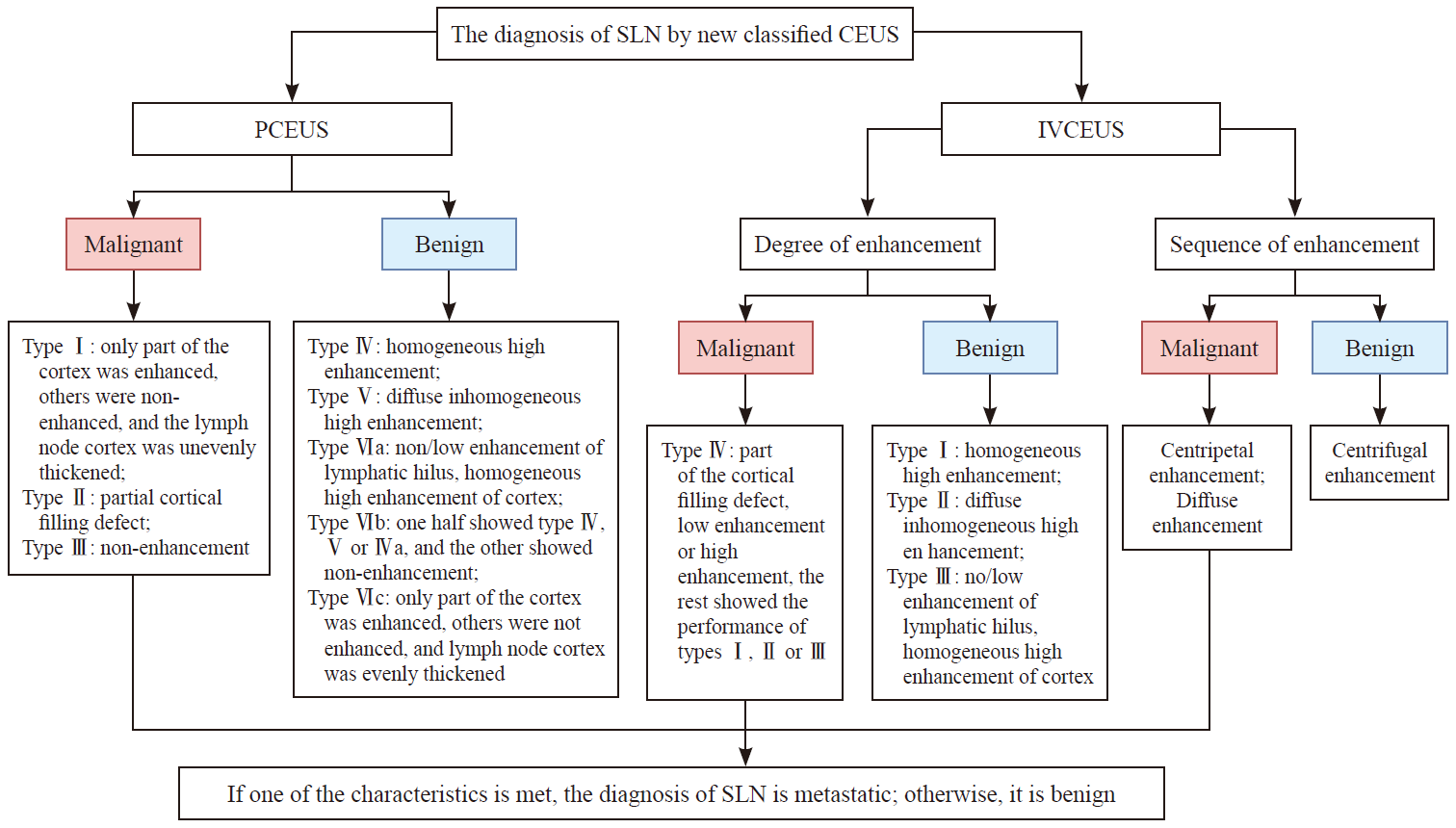
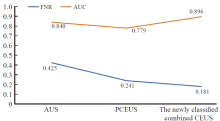
图3
几种超声方法的FNR和AUC"
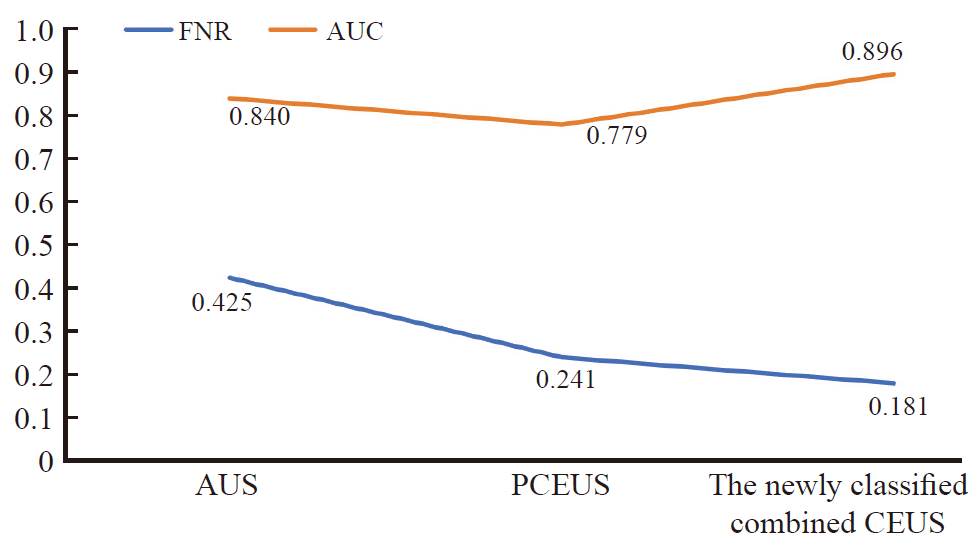
表1
不同影像学技术FNR和诊断效能"
| Imaging technology | FNR/% | Sensitivity/% | Specificity/% | Diagnostic limitation |
|---|---|---|---|---|
| PET/CT | 62 | 38 | 86 | Small residual lymph nodes are insensitive to FDG uptake |
| MRI | 40 | 60 | 76 | The axilla may be insufficiently covered; depending on the pathological subtype of the primary lesion |
| Ultrasound | 26.1 | 73.9 | 100 | The accuracy is insufficient when used alone |
| CEUS+BD | 15.6 | 84.4 | 100 | SLN structural characteristics are not combined; the classification is simple |
| [1] | SIEGEL R L, GIAQUINTO A N, JEMAL A. Cancer statistics, 2024[J]. CA A Cancer J Clinicians, 2024, 74(1): 12-49. |
| [2] |
《中国乳腺癌新辅助治疗专家共识(2022年版)》专家组. 中国乳腺癌新辅助治疗专家共识(2022年版)[J]. 中国癌症杂志, 2022, 32(1): 80-88.
doi: 10.19401/j.cnki.1007-3639.2022.01.011 |
| Expert group of expert consensus on neoadjuvant treatment of breast cancer in China (2022 edition). Expert consensus on neoadjuvant treatment of breast cancer in China (2022 edition)[J]. China Oncol, 2022, 32(1): 80-88. | |
| [3] |
FERRARAZZO G, NIERI A, FIRPO E, et al. The role of sentinel lymph node biopsy in breast cancer patients who become clinically node-negative following neo-adjuvant chemotherapy: a literature review[J]. Curr Oncol, 2023, 30(10): 8703-8719.
doi: 10.3390/curroncol30100630 pmid: 37887530 |
| [4] | SHIRZADI A, MAHMOODZADEH H, QORBANI M. Assessment of sentinel lymph node biopsy after neoadjuvant chemotherapy for breast cancer in two subgroups: initially node negative and node positive converted to node negative-a systemic review and meta-analysis[J]. J Res Med Sci, 2019, 24: 18. |
| [5] | VÁZQUEZ J C, PIÑERO A, DE CASTRO F J, et al. The value of sentinel lymph-node biopsy in women with node-positive breast cancer at diagnosis and node-negative tumour after neoadjuvant therapy: a systematic review[J]. Clin Transl Oncol, 2023, 25(2): 417-428. |
| [6] |
BOUGHEY J C, SUMAN V J, MITTENDORF E A, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (alliance) clinical trial[J]. JAMA, 2013, 310(14): 1455-1461.
doi: 10.1001/jama.2013.278932 pmid: 24101169 |
| [7] | BOILEAU J F, POIRIER B, BASIK M, et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: the SN FNAC study[J]. J Clin Oncol, 2015, 33(3): 258-264. |
| [8] |
KUEHN T, BAUERFEIND I, FEHM T, et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): a prospective, multicentre cohort study[J]. Lancet Oncol, 2013, 14(7): 609-618.
doi: 10.1016/S1470-2045(13)70166-9 pmid: 23683750 |
| [9] | CAO S Y, LIU X, CUI J W, et al. Feasibility and reliability of sentinel lymph node biopsy after neoadjuvant chemotherapy in breast cancer patients with positive axillary nodes at initial diagnosis: an up-to-date meta-analysis of 3, 578 patients[J]. Breast, 2021, 59: 256-269. |
| [10] | KRAG D N, ANDERSON S J, JULIAN T B, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase Ⅲ trial[J]. Lancet Oncol, 2007, 8(10): 881-888. |
| [11] | SAMIEI S, SIMONS J M, ENGELEN S M E, et al. Axillary pathologic complete response after neoadjuvant systemic therapy by breast cancer subtype in patients with initially clinically node-positive disease: a systematic review and meta-analysis[J]. JAMA Surg, 2021, 156(6): e210891. |
| [12] |
毕钊, 陈鹏, 邱鹏飞, 等. 乳腺癌新辅助治疗后腋窝淋巴结转移情况分析[J]. 中国癌症杂志, 2023, 33(4): 361-367.
doi: 10.19401/j.cnki.1007-3639.2023.04.006 |
| BI Z, CHEN P, QIU P F, et al. The analysis of axillary lymph nodes metastasis after neoadjuvant therapy in breast cancer[J]. China Oncol, 2023, 33(4): 361-367. | |
| [13] | VAN HEMERT A K E, VAN LOEVEZIJN A A, BAAS M P D, et al. Omitting axillary lymph node dissection in breast cancer patients with extensive nodal disease and excellent response to primary systemic therapy using the MARI protocol[J]. Breast, 2025, 80: 104411. |
| [14] |
DONKER M, STRAVER M E, WESSELING J, et al. Marking axillary lymph nodes with radioactive iodine seeds for axillary staging after neoadjuvant systemic treatment in breast cancer patients: the MARI procedure[J]. Ann Surg, 2015, 261(2): 378-382.
doi: 10.1097/SLA.0000000000000558 pmid: 24743607 |
| [15] |
VAN DER NOORDAA M M, VAN DUIJNHOVEN F H, STRAVER M E, et al. Major reduction in axillary lymph node dissections after neoadjuvant systemic therapy for node-positive breast cancer by combining PET/CT and the MARI procedure[J]. Ann Surg Oncol, 2018, 25(6): 1512-1520.
doi: 10.1245/s10434-018-6404-y pmid: 29511992 |
| [16] | VAN LOEVEZIJN A A, VAN DER NOORDAA M E M, STOKKEL M P M, et al. Three-year follow-up of de-escalated axillary treatment after neoadjuvant systemic therapy in clinically node-positive breast cancer: the MARI-protocol[J]. Breast Cancer Res Treat, 2022, 193(1): 37-48. |
| [17] | ARAGÓN-SÁNCHEZ S, CIRUELOS-GIL E, LÓPEZ-MARÍN L, et al. Feasibility of targeted axillary dissection for de-escalation of surgical treatment after neoadjuvant chemotherapy in breast cancer[J]. Surg Oncol, 2022, 44: 101823. |
| [18] | WU S Y, LI J W, WANG Y J, et al. Clinical feasibility and oncological safety of non-radioactive targeted axillary dissection after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: a prospective diagnostic and prognostic study[J]. Int J Surg, 2023, 109(7): 1863-1870. |
| [19] | CABıOĞLU N, KARANLıK H, YıLMAZ R, et al. Targeted axillary dissection reduces residual nodal disease in clinically node- positive breast cancer after neoadjuvant chemotherapy[J]. World J Surg Oncol, 2024, 22(1): 178. |
| [20] |
LAWS A, LEONARD S, VINCUILLA J, et al. Risk of surgical overtreatment in CN1 breast cancer patients who become ypN0 after neoadjuvant chemotherapy: SLNB versus TAD[J]. Ann Surg Oncol, 2025, 32(3): 2023-2028.
doi: 10.1245/s10434-024-16625-7 pmid: 39633166 |
| [21] |
SIMONS J M, VAN NIJNATTEN T J A, VAN DER POL C C, et al. Diagnostic accuracy of radioactive iodine seed placement in the axilla with sentinel lymph node biopsy after neoadjuvant chemotherapy in node-positive breast cancer[J]. JAMA Surg, 2022, 157(11): 991-999.
doi: 10.1001/jamasurg.2022.3907 pmid: 36069889 |
| [22] |
VAN NIJNATTEN T J A, SIMONS J M, SMIDT M L, et al. A novel less-invasive approach for axillary staging after neoadjuvant chemotherapy in patients with axillary node-positive breast cancer by combining radioactive iodine seed localization in the axilla with the sentinel node procedure (RISAS): a Dutch prospective multicenter validation study[J]. Clin Breast Cancer, 2017, 17(5): 399-402.
doi: S1526-8209(17)30130-1 pmid: 28487053 |
| [23] | BOUGHEY J C, YU H M, DUGAN C L, et al. Changes in surgical management of the axilla over 11 years-report on more than 1500 breast cancer patients treated with neoadjuvant chemotherapy on the prospective I-SPY2 trial[J]. Ann Surg Oncol, 2023, 30(11): 6401-6410. |
| [24] | HEIDINGER M, WEBER W P. Axillary surgery for breast cancer in 2024[J]. Cancers (Basel), 2024, 16(9): 1623. |
| [25] |
中国抗癌协会乳腺癌专业委员会, 中华医学会肿瘤学分会乳腺肿瘤学组. 中国抗癌协会乳腺癌诊治指南与规范(2024年版)[J]. 中国癌症杂志, 2023, 33(12): 1092-1187.
doi: 10.19401/j.cnki.1007-3639.2023.12.004 |
| The Society of Breast Cancer China Anti-Cancer Association, Breast Oncology Group of the Oncology Branch of the Chinese Medical Association. Guidelines for breast cancer diagnosis and treatment by China Anti-cancer Association (2024 edition)[J]. China Oncol, 2023, 33(12): 1092-1187. | |
| [26] | AMIN M B, EDGE S B, GREENE F L, et al. AJCC cancer staging manual[M]. 8th ed. New York: Springer, 2017: 589-636. |
| [27] | LEE J, PARK S, BAE S J, et al. Micrometastases in axillary lymph nodes in breast cancer, post-neoadjuvant systemic therapy[J]. Breast Cancer Res, 2024, 26(1): 120. |
| [28] |
CABIOĞLU N, KARANLIK H, YILDIRIM N, et al. Favorable outcome with sentinel lymph node biopsy alone after neoadjuvant chemotherapy in clinically node positive breast cancer at diagnosis: Turkish multicentric NEOSENTI-TURK MF-18-02-study[J]. Eur J Surg Oncol, 2021, 47(10): 2506-2514.
doi: 10.1016/j.ejso.2021.06.024 pmid: 34217580 |
| [29] | HOUVENAEGHEL G, COHEN M, RARO P, et al. Sentinel node involvement with or without completion axillary lymph node dissection: treatment and pathologic results of randomized SERC trial[J]. NPJ Breast Cancer, 2021, 7(1): 133. |
| [30] |
WONG S M, ALMANA N, CHOI J, et al. Prognostic significance of residual axillary nodal micrometastases and isolated tumor cells after neoadjuvant chemotherapy for breast cancer[J]. Ann Surg Oncol, 2019, 26(11): 3502-3509.
doi: 10.1245/s10434-019-07517-2 pmid: 31228134 |
| [31] | MOO T A, EDELWEISS M, HAJIYEVA S, et al. Is low-volume disease in the sentinel node after neoadjuvant chemotherapy an indication for axillary dissection?[J]. Ann Surg Oncol, 2018, 25(6): 1488-1494. |
| [32] | CLASSE J M, LOAEC C, GIMBERGUES P, et al. Sentinel lymph node biopsy without axillary lymphadenectomy after neoadjuvant chemotherapy is accurate and safe for selected patients: the GANEA 2 study[J]. Breast Cancer Res Treat. 2019 ;173(2):343-352. |
| [33] | LIN S Q, VO N P, YEN Y C, et al. Outcomes of sentinel node biopsy for women with breast cancer after neoadjuvant therapy: systematic review and meta-analysis of real-world data[J]. Ann Surg Oncol, 2022, 29(5): 3038-3049. |
| [34] | ZAHWE M, GHZAIEL A, NAJIA A, et al. Performance of sentinel lymph node biopsy after neoadjuvant chemotherapy in clinically node-positive breast cancer patients: systematic review and meta-analysis[J]. Int J Surg, 2025, 111(4): 3040-3050. |
| [35] | FU J F, CHEN H L, YANG J, et al. Feasibility and accuracy of sentinel lymph node biopsy in clinically node-positive breast cancer after neoadjuvant chemotherapy: a meta-analysis[J]. PLoS One, 2014, 9(9): e105316. |
| [36] |
SAMIEI S, DE MOOIJ C M, LOBBES M B I, et al. Diagnostic performance of noninvasive imaging for assessment of axillary response after neoadjuvant systemic therapy in clinically node-positive breast cancer: a systematic review and meta-analysis[J]. Ann Surg, 2021, 273(4): 694-700.
doi: 10.1097/SLA.0000000000004356 pmid: 33201095 |
| [37] | LUAN T, LI Y Q, WU Q W, et al. Value of quantitative SPECT/CT lymphoscintigraphy in improving sentinel lymph node biopsy in breast cancer[J]. Breast J, 2022, 2022: 6483318. |
| [38] |
CHRISTIN O L, KUTEN J, EVEN-SAPIR E, et al. Node positive breast cancer: concordance between baseline PET/CT and sentinel node assessment after neoadjuvant therapy[J]. Surg Oncol, 2019, 30: 1-5.
doi: S0960-7404(19)30066-0 pmid: 31500769 |
| [39] | BAE S J, CHUN J W, LEE S B, et al. Outcomes of sentinel node biopsy according to MRI response in an association with the subtypes in CN1-3 breast cancer after neoadjuvant systemic therapy, multicenter cohort study[J]. Breast Cancer Res, 2024, 26(1): 66. |
| [40] | DI MICCO R, SANTURRO L, GASPARRI M L, et al. PET/MRI for staging the axilla in breast cancer: current evidence and the rationale for SNB vs PET/MRI trials[J]. Cancers (Basel), 2021, 13(14): 3571. |
| [41] | QUINLAN C, UYEDA J W. Patient-friendly summary of the ACR appropriateness criteria: monitoring response to neoadjuvant systemic therapy for breast cancer[J]. J Am Coll Radiol, 2018, 15(7): e11. |
| [42] | LEINERT E, LUKAC S, SCHWENTNER L, et al. The use of axillary ultrasound (AUS) to assess the nodal status after neoadjuvant chemotherapy (NACT) in primary breast cancer patients[J]. Surg Oncol, 2024, 52: 102016. |
| [43] | LIU Y, WANG Y, FENG S W, et al. Axillary ultrasound after neoadjuvant therapy reduces the false-negative rate of sentinel lymph node biopsy in patients with cytologically node-positive breast cancer[J]. Breast Cancer Res Treat, 2023, 197(3): 515-523. |
| [44] | 牛向阳, 冯其贞, 熊斌. 各种示踪技术在乳腺癌前哨淋巴结的应用进展[J]. 临床医学进展, 2024, 14(7): 870-876. |
| NIU X Y, FENG Q Z, XIONG B. Application progress of various tracer techniques in sentinel lymph node of breast cancer[J]. Adv Clin Med, 2024, 14(7): 870-876. | |
| [45] | 董维露, 蔡婷, 许华宁, 等. 乳腺癌前哨淋巴结经皮淋巴管超声造影结合临床病理特征的Logistic回归分析[J]. 中华超声影像学杂志, 2023, 32(12): 1083-1089. |
| DONG W L, CAI T, XU H N, et al. Regression analysis of percutaneous lymphatic contrast-enhanced ultrasound combined with clinicopathological features in the diagnosis of sentinel lymph nodes in breast cancer[J]. Chin J Ultrasonogr, 2023, 32(12): 1083-1089. | |
| [46] | ZHENG Y, SUN J, ZHU L, et al. Diagnosing sentinel lymph node metastasis of T1/T2 breast cancer with conventional ultrasound combined with double contrast-enhanced ultrasound: a preliminary study[J]. Quant Imaging Med Surg, 2023, 13(6): 3451-3463. |
| [47] | LI J, LI H, GUAN L, et al. The value of preoperative sentinel lymph node contrast-enhanced ultrasound for breast cancer: a large, multicenter trial[J]. BMC Cancer, 2022, 22(1): 455. |
| [48] | HUANG C X, LUO J, SHAN Z, et al. The value of the improved percutaneous and intravenous contrast-enhanced ultrasound diagnostic classification in sentinel lymph nodes of breast cancer[J]. Quant Imaging Med Surg, 2024, 14(3): 2391-2404. |
| [49] |
WU X F, TANG L N, HUANG W Q, et al. Contrast-enhanced ultrasonography and blue dye methods in detection of sentinel lymph nodes following neoadjuvant chemotherapy in initially node positive breast cancer[J]. Arch Gynecol Obstet, 2020, 302(3): 685-692.
doi: 10.1007/s00404-020-05646-8 pmid: 32602000 |
| [1] | 王孟潇, 樊文栋, 曹菁璟, 陈佳艺, 蔡钢, 曹璐. 基于每日CBCT的乳腺癌术后单周超大分割全乳放疗的位置误差及外扩边界研究[J]. 中国癌症杂志, 2025, 35(8): 752-760. |
| [2] | 吴佳辰, 何丽娜, 汤鑫茹, 唐爽. Ptenfl/fl;Trp53fl/fl;Pbsn-iCre+基因编辑小鼠自发形成前列腺癌与乳腺癌的模型构建研究[J]. 中国癌症杂志, 2025, 35(8): 769-775. |
| [3] | 吕刚, 王光庆, 郑炎, 唐琴, 陈飞, 俞旭东, 许盛琪, 汤发扬, 朱际飚. 吲哚菁绿在乳腺癌手术切缘评估和范围定位中的有效性、安全性探索:一项单中心、观察性队列研究[J]. 中国癌症杂志, 2025, 35(8): 776-783. |
| [4] | 翟梓涵, 陈盛. MRI预测乳腺癌淋巴结状态的研究进展及展望[J]. 中国癌症杂志, 2025, 35(8): 799-807. |
| [5] | 李心翔, 骆大葵. 直肠癌外科治疗的创新模式探讨[J]. 中国癌症杂志, 2025, 35(7): 631-636. |
| [6] | 张钰洋, 刘骞. 结直肠癌新辅助免疫治疗的进展与展望[J]. 中国癌症杂志, 2025, 35(7): 642-656. |
| [7] | 钱佳佳, 阮聪, 刘继勇, 徐蕊. 免疫检查点抑制剂在肢端型黑色素瘤治疗中的研究进展[J]. 中国癌症杂志, 2025, 35(7): 702-709. |
| [8] | 王红霞, 殷咏梅, 胡夕春. 中国乳腺癌患者BRCA1/2基因检测与临床应用专家共识(2025年版)[J]. 中国癌症杂志, 2025, 35(7): 710-734. |
| [9] | 钱芳, 孙永强, 张思涵, 宋田利. 乳腺癌改良根治术后感染的病原学特征、影响因素及炎症因子分析[J]. 中国癌症杂志, 2025, 35(6): 563-569. |
| [10] | 鲍正敏, 李乾永, 鲁晓腾, 杨彦举. 分次内CBCT影像引导技术引入DIBH在左侧乳腺癌放疗中的意义[J]. 中国癌症杂志, 2025, 35(6): 578-584. |
| [11] | 杜心悦, 邬思雨, 柳光宇. 乳腺癌术后孤立腋窝淋巴结复发的临床特征与治疗进展[J]. 中国癌症杂志, 2025, 35(6): 592-600. |
| [12] | 张钰佳, 马力. 乳腺癌外科治疗领域新技术的进展和争议[J]. 中国癌症杂志, 2025, 35(4): 339-345. |
| [13] | 胡玮, 任晓朦, 王洋, 赵培庆, 曹凯. TIPE通过调控LDHA表达影响三阴性乳腺癌糖代谢重编程机制研究[J]. 中国癌症杂志, 2025, 35(4): 386-393. |
| [14] | 贾瑞杰, 石志强, 张琦, 逯永晋, 郑竣升, 孙菁, 毕钊, 孙晓, 王永胜, 邱鹏飞. 乳腺癌内乳前哨淋巴结活检与患者预后的相关性研究[J]. 中国癌症杂志, 2025, 35(4): 394-403. |
| [15] | 薛佳磊, 李剑伟, 龚悦, 柳光宇, 刘哲斌. 早期乳腺癌术中快速冰冻切片病理学检查延迟诊断率分析:一项真实世界的回顾性研究[J]. 中国癌症杂志, 2025, 35(4): 404-411. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
地址:上海市徐汇区东安路270号复旦大学附属肿瘤医院10号楼415室
邮编:200032 电话:021-64188274 E-mail:zgazzz@china-oncology.com
访问总数:; 今日访问总数:; 当前在线人数:
本系统由北京玛格泰克科技发展有限公司设计开发 技术支持:support@magtech.com.cn