Welcome to China Oncology,
China Oncology ›› 2025, Vol. 35 ›› Issue (8): 752-760.doi: 10.19401/j.cnki.1007-3639.2025.08.003
• Article • Previous Articles Next Articles
WANG Mengxiao1( ), FAN Wendong2(), CAO Jingjing1, CHEN Jiayi1,2, CAI Gang2(), CAO Lu1()
), FAN Wendong2(), CAO Jingjing1, CHEN Jiayi1,2, CAI Gang2(), CAO Lu1()
Received:2025-03-04
Revised:2025-06-05
Online:2025-08-30
Published:2025-09-10
Contact:
CAI Gang, CAO Lu
Supported by:Share article
CLC Number:
WANG Mengxiao, FAN Wendong, CAO Jingjing, CHEN Jiayi, CAI Gang, CAO Lu. Set-up error and CTV margin in one-week ultra-hypofractionated whole breast irradiation after breast-conserving surgery based on daily CBCT[J]. China Oncology, 2025, 35(8): 752-760.
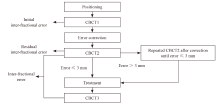
Fig. 1
Flowchart of CBCT imaging guidance"
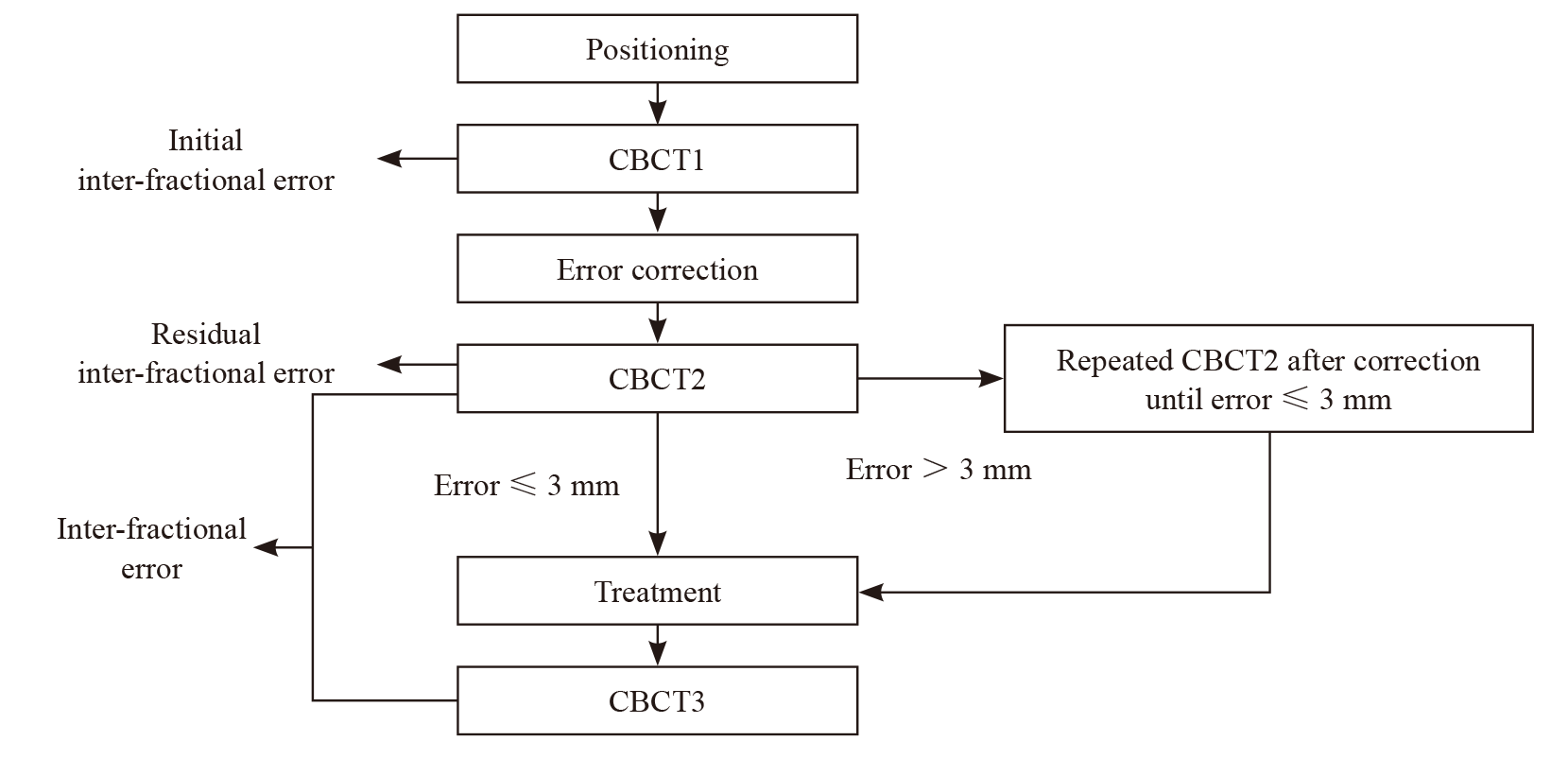

Fig. 2
Calculation of Σ and σ of inter-fractional and intra-fractional error M: Mean; SD: Standard deviation; RMS: Root mean square."
Tab. 1
Clinicopathological characteristics of the patients"
| Characteristics | Patients (n=34) |
|---|---|
| Age median (range)/year | 53.5 (40.0, 74.0) |
| CTV volume median (range)/cm3 | 402.5 (143.2, 958.6) |
| Height median (range)/cm | 161.5 (150.0, 168.0) |
| Weight median (range)/kg | 60.0 (45.0, 78.0) |
| BMI median (range)/ (kg·m-2) | 23.2 (18.0, 28.0) |
| Laterality n(%) | |
| Left | 22 (64.7) |
| Right | 12 (35.3) |
| Quadrant n(%) | |
| Upper inner | 6 (17.6) |
| Lower inner | 4 (11.8) |
| Upper outer | 20 (58.8) |
| Lower outer | 4 (11.8) |
| Axillary surgery n(%) | |
| Sentinel lymph node biopsy | 32 (94.1) |
| None | 2 (5.9) |
| Pathological tumor stage n(%) | |
| pTis | 6 (17.6) |
| pT1 | 24 (70.6) |
| pT2 | 4 (11.8) |
| Pathological nodal stage n(%) | |
| pNx | 2 (5.9) |
| pN0 | 31 (91.2) |
| pN1mi | 1 (2.9) |
| Subtype n(%) | |
| HR+/HER2+ | 2 (5.9) |
| HR+/HER2- | 27 (79.4) |
| HR-/HER2+ | 1 (2.9) |
| HR-/HER2- | 4 (11.8) |
| Adjuvant therapy n(%) | |
| None | 19 (55.8) |
| Chemotherapy | 12 (35.3) |
| Chemotherapy+anti-HER2 therapy | 3 (8.8) |
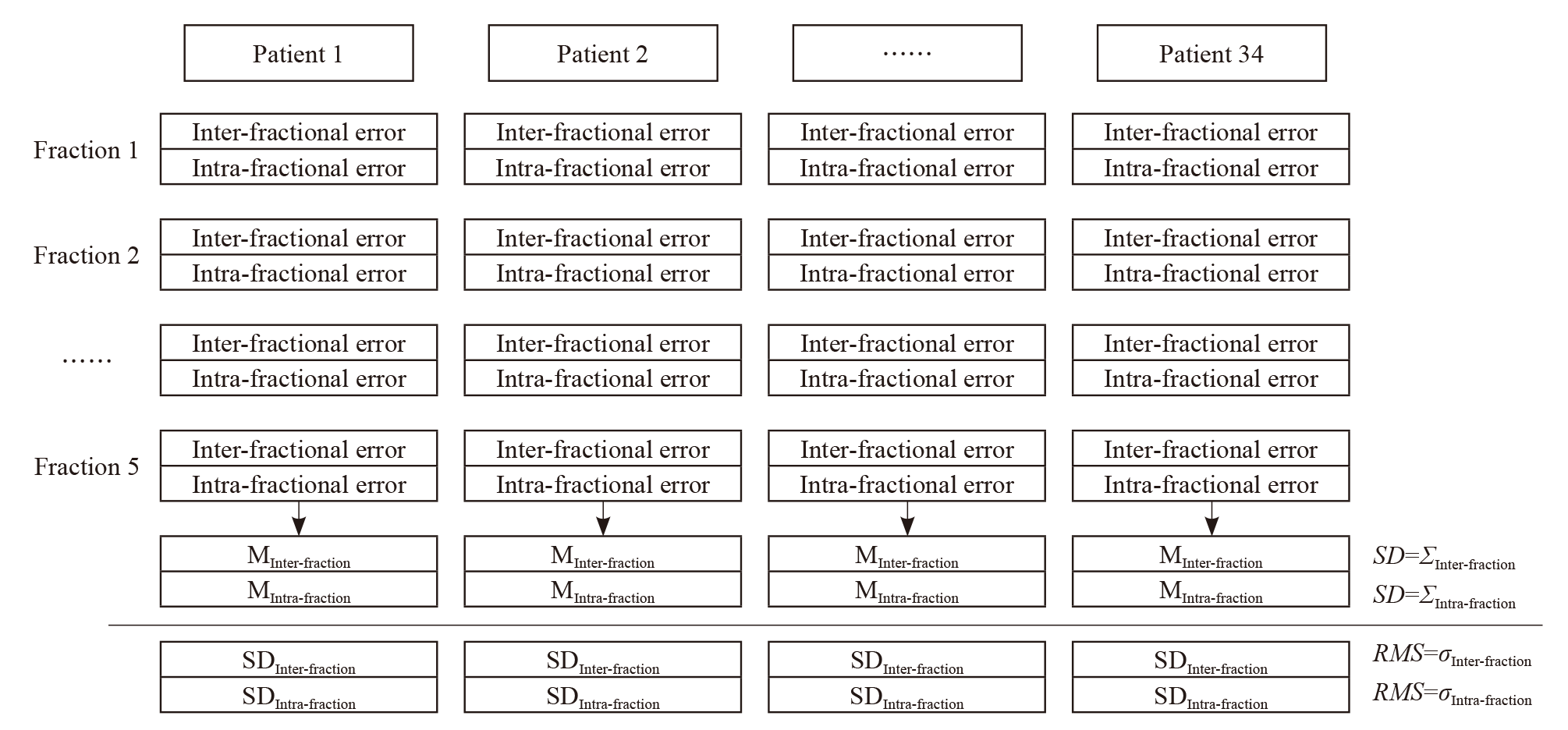
Fig. 3
Flowchart of patients inclusion and exclusion"

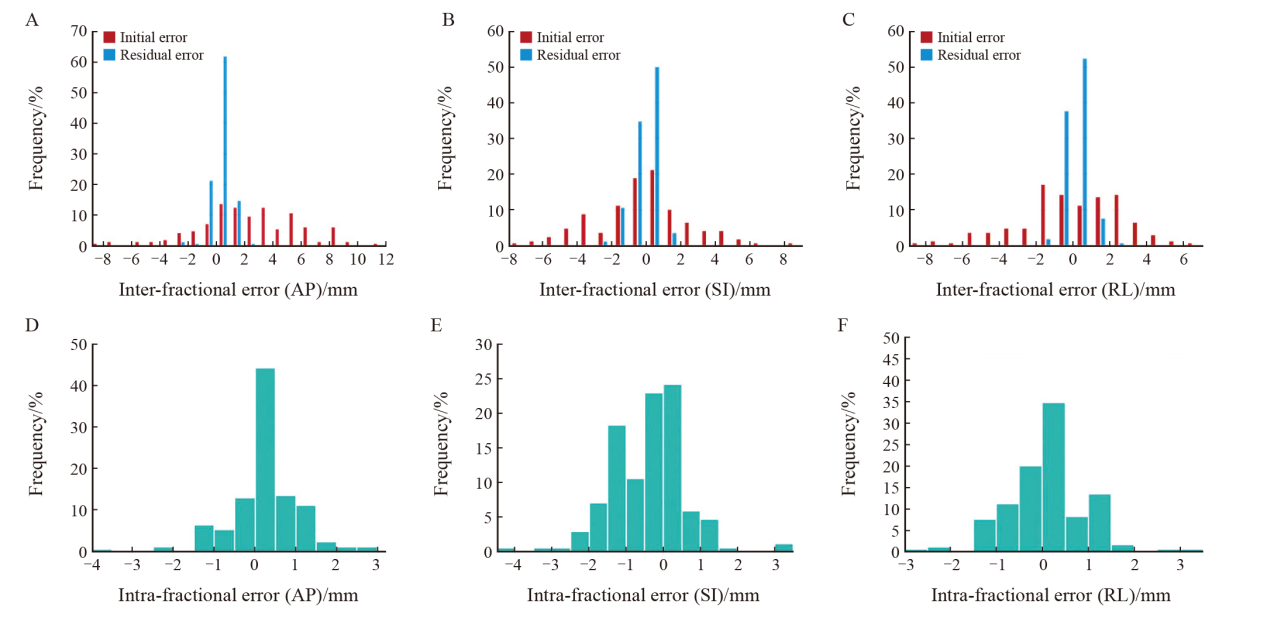
Fig. 4
Distributions of inter-fractional and intra-fractional errors of 170 fractions in overall cohort A-C: Distributions of initial and residual inter-fractional errors in anterior-posterior (AP), superior-inferior (SI) and right-left (RL) directions. D-F: Distributions of intra-fractional errors in AP, SI or RL directions."
Tab. 2
Comparison of residual inter-fractional error between patients with different clinical characteristics."
| AP/mm | SI/mm | RL/mm | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (range) | Z valuea/ H valueb | P value | Median (range) | Z value/ H value | P value | Median (range) | Z value/ H value | P value | |||
| Age/year | -0.818 | 0.414 | -0.335 | 0.738 | -0.003 | 0.997 | |||||
| ≤53.5 | 0.5 (0.0, 2.1) | 0.5 (0.0, 2.1) | 0.3 (0.0, 2.6) | ||||||||
| >53.5 | 0.4 (0.0, 2.4) | 0.5 (0.2, 2.0) | 0.3 (0.0, 1.9) | ||||||||
| CTV/cm3 | -2.265 | 0.023 | -2.083 | 0.037 | -1.587 | 0.112 | |||||
| ≤402.5 | 0.3 (0.0, 2.4) | 0.5 (0.0, 2.0) | 0.4 (0.0, 2.6) | ||||||||
| >402.5 | 0.5 (0.0, 2.1) | 0.6 (0.0, 2.1) | 0.2 (0.0, 1.9) | ||||||||
| Height/cm | -2.206 | 0.027 | -0.770 | 0.441 | -0.480 | 0.631 | |||||
| ≤161.5 | 0.4 (0.0, 2.1) | 0.5 (0.0, 2.1) | 0.2 (0.0, 2.6) | ||||||||
| >161.5 | 0.4 (0.0, 2.4) | 0.5 (0.0, 2.0) | 0.3 (0.0, 1.9) | ||||||||
| Weight/kg | -0.839 | 0.401 | -0.804 | 0.421 | -0.710 | 0.478 | |||||
| ≤60.0 | 0.4 (0.0, 2.4) | 0.5 (0.0, 2.1) | 0.4 (0.0, 2.6) | ||||||||
| >60.0 | 0.5 (0.0, 2.1) | 0.5 (0.0, 1.9) | 0.2 (0.0, 1.9) | ||||||||
| BMI/(kg·m-2) | -0.252 | 0.801 | -1.701 | 0.089 | -0.848 | 0.396 | |||||
| ≤23.2 | 0.4 (0.0, 2.4) | 0.5 (0.0, 2.0) | 0.4 (0.0, 2.6) | ||||||||
| >23.2 | 0.4 (0.0, 2.1) | 0.5 (0.0, 2.1) | 0.3 (0.0, 1.9) | ||||||||
| Laterality | -0.987 | 0.324 | -1.299 | 0.194 | -1.520 | 0.129 | |||||
| Left | 0.4 (0.0, 2.1) | 0.5 (0.0, 1.9) | 0.3 (0.0, 2.6) | ||||||||
| Right | 0.6 (0.0, 2.4) | 0.5 (0.1, 2.1) | 0.4 (0.0, 1.9) | ||||||||
| Quadrant | 1.862 | 0.601 | 7.222 | 0.065 | 2.754 | 0.431 | |||||
| Upper inner | 0.5 (0.0, 2.4) | 0.5 (0.0, 2.0) | 0.4 (0.0, 2.6) | ||||||||
| Lower inner | 0.5 (0.0, 1.3) | 0.8 (0.1, 1.8) | 0.2 (0.0, 0.9) | ||||||||
| Upper outer | 0.4 (0.0, 2.1) | 0.5 (0.0, 2.1) | 0.4 (0.0, 1.9) | ||||||||
| Lower outer | 0.4 (0.1, 2.1) | 0.8 (0.0, 1.9) | 0.3 (0.0, 1.0) | ||||||||
| Adjuvant therapy | -1.495 | 0.135 | -1.414 | 0.157 | -0.370 | 0.711 | |||||
| None | 0.4 (0.0, 2.1) | 0.5 (0.0, 2.1) | 0.3 (0.0, 2.6) | ||||||||
| Yes | 0.5 (0.0, 2.4) | 0.6 (0.0, 2.0) | 0.3 (0.0, 1.4) | ||||||||
Tab. 3
Comparison of intra-fractional error between patients with different clinical characteristics"
| Item | AP/mm | SI/mm | RL/mm | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (range) | Z valuea/ H valueb | P value | Median (range) | Z value/ H value | P value | Median (range) | Z value/ H value | P value | |||
| Age/year | -1.109 | 0.267 | -0.713 | 0.476 | -0.743 | 0.457 | |||||
| ≤53.5 | 0.2 (0.0, 3.9) | 0.8 (0.0, 4.4) | 0.5 (0.0, 3.1) | ||||||||
| >53.5 | 0.4 (0.0, 2.6) | 0.6 (0.0, 3.0) | 0.2 (0.0, 2.8) | ||||||||
| CTV/cm3 | -3.308 | 0.001 | -1.286 | 0.198 | -1.156 | 0.248 | |||||
| ≤402.5 | 0.2 (0.0, 2.4) | 0.5 (0.0, 4.4) | 0.2 (0.0, 3.1) | ||||||||
| >402.5 | 0.5 (0.0, 3.9) | 0.9 (0.0, 3.5) | 0.4 (0.0, 2.5) | ||||||||
| Height/cm | -1.329 | 0.184 | -0.347 | 0.729 | -0.555 | 0.579 | |||||
| ≤161.5 | 0.2 (0.0, 3.9) | 0.6 (0.0, 4.4) | 0.3 (0.0, 3.1) | ||||||||
| >161.5 | 0.4 (0.0, 2.6) | 0.7 (0.0, 3.5) | 0.3 (0.0, 2.2) | ||||||||
| Weight/kg | -2.129 | 0.033 | -0.461 | 0.645 | -0.597 | 0.550 | |||||
| ≤60.0 | 0.2 (0.0, 3.9) | 0.7 (0.0, 4.4) | 0.3 (0.0, 3.1) | ||||||||
| >60.0 | 0.5 (0.0, 2.6) | 0.6 (0.0, 3.5) | 0.5 (0.0, 1.9) | ||||||||
| BMI/(kg·m-2) | -3.506 | <0.001 | -1.624 | 0.104 | -1.501 | 0.133 | |||||
| ≤23.2 | 0.2 (0.0, 2.3) | 0.5 (0.0, 3.5) | 0.3 (0.0, 3.1) | ||||||||
| >23.2 | 0.7 (0.0, 3.9) | 0.8 (0.0, 4.4) | 0.5 (0.0, 2.5) | ||||||||
| Laterality | -0.350 | 0.726 | -1.571 | 0.116 | -1.692 | 0.091 | |||||
| Left | 0.3 (0.0, 2.5) | 0.6 (0.0, 3.0) | 0.6 (0.0, 3.1) | ||||||||
| Right | 0.3 (0.0, 3.9) | 0.9 (0.0, 4.4) | 0.2 (0.0, 2.8) | ||||||||
| Quadrant | 1.336 | 0.721 | 10.375 | 0.016 | 7.106 | 0.069 | |||||
| Upper inner | 0.2 (0.0, 1.1) | 0.3 (0.0, 2.4) | 0.2 (0.0, 2.2) | ||||||||
| Lower inner | 0.2 (0.0, 2.4) | 1.3 (0.0, 4.4) | 0.3 (0.0, 1.5) | ||||||||
| Upper outer | 0.3 (0.0, 3.9) | 0.5 (0.0, 3.0) | 0.5 (0.0, 3.1) | ||||||||
| Lower outer | 0.3 (0.0, 2.2) | 0.9 (0.0, 3.0) | 0.9 (0.0, 1.9) | ||||||||
| Adjuvant therapy | -0.297 | 0.766 | -1.841 | 0.066 | -0.224 | 0.823 | |||||
| None | 0.2 (0.0, 3.9) | 0.8 (0.0, 4.4) | 0.3 (0.0, 3.1) | ||||||||
| Yes | 0.4 (0.0, 2.3) | 0.3 (0.0, 3.5) | 0.3 (0.0, 2.2) | ||||||||
Tab. 4
CTV to PTV margin in single-week ultra-hypofractionated whole breast irradiation"
| Item | Margin without daily CBCT/mm | Margin with daily CBCT/mm | |||||
|---|---|---|---|---|---|---|---|
| AP | SI | RL | AP | SI | RL | ||
| Overall cohort (n=34) | 8.9 | 7.2 | 7.1 | 2.3 | 2.8 | 2.0 | |
| Categorized by BMI | |||||||
| ≤23.2kg/m2 (n=17) | 9.0 | 6.3 | 5.6 | 1.8 | 2.3 | 2.0 | |
| >23.2kg/m2 (n=17) | 8.6 | 7.9 | 8.4 | 2.6 | 3.4 | 2.0 | |
| Categorized by height | |||||||
| ≤161.5 cm (n=17) | 8.6 | 4.6 | 6.8 | 2.2 | 2.7 | 2.3 | |
| >161.5 cm (n=17) | 9.2 | 8.6 | 7.5 | 2.3 | 2.9 | 1.8 | |
| Categorized by weight | |||||||
| ≤60.0 kg (n=19) | 8.7 | 6.2 | 6.0 | 2.2 | 2.7 | 2.2 | |
| >60.0 kg (n=15) | 9.2 | 8.2 | 8.2 | 2.4 | 2.9 | 1.7 | |
| Categorized by CTV | |||||||
| ≤402.5 cm3 (n=17) | 6.8 | 6.4 | 5.9 | 1.6 | 2.6 | 2.1 | |
| >402.5 cm3 (n=17) | 10.1 | 8.0 | 8.2 | 2.8 | 3.1 | 2.0 | |
| Categorized by quadrant | |||||||
| Upper inner quadrant (n=6) | 6.5 | 5.5 | 5.1 | 1.8 | 2.2 | 2.0 | |
| Lower inner quadrant (n=4) | 10.7 | 5.8 | 4.5 | 1.8 | 2.5 | 1.8 | |
| Upper outer quadrant (n=20) | 9.1 | 7.7 | 7.5 | 2.2 | 2.6 | 2.1 | |
| Lower outer quadrant (n=4) | 7.3 | 7.8 | 7.5 | 2.9 | 4.2 | 2.1 | |
| [1] | Early Breast Cancer Trialists; Collaborative Group (EBCTCG), DARBY S, MCGALE P, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10 801 women in 17 randomised trials[J]. Lancet, 2011, 378(9804): 1707-1716. |
| [2] |
BRUNT A M, HAVILAND J S, WHEATLEY D A, et al. Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial[J]. Lancet, 2020, 395(10237): 1613-1626.
doi: S0140-6736(20)30932-6 pmid: 32580883 |
| [3] | 杨伟志, 冯宁远, 沈瑜. LQ公式的生物学概念及应用[J]. 中华放射肿瘤学杂志, 1995, 4(2): 59-63. |
| YANG W Z, FENG N Y, SHEN Y. Biological concept and application of LQ formula[J]. Chin J Radiat Oncol, 1995, 4(2): 59-63. | |
| [4] |
VAN H M. Errors and margins in radiotherapy[J]. Semin Radiat Oncol, 2004, 14(1): 52-64.
doi: 10.1053/j.semradonc.2003.10.003 pmid: 14752733 |
| [5] |
LEE J, LIU S H, LIN J B, et al. Image-guided study of inter-fraction and intra-fraction set-up variability and margins in reverse semi-decubitus breast radiotherapy[J]. Radiat Oncol, 2018, 13(1): 254.
doi: 10.1186/s13014-018-1200-1 pmid: 30587208 |
| [6] | SIGAUDI V, ZANNETTI M, FERRARA E, et al. Ultra-hypofractionation for whole-breast irradiation in early breast cancer: interim analysis of a prospective study[J]. Biomedicines, 2022, 10(10): 2568. |
| [7] | IVANOV O, MILOVANČEV A, PETROVIĆ B, et al. Ultra-hypofractionated vs moderate fractionated whole breast three dimensional conformal radiotherapy during the COVID-19 pandemic[J]. Medicina (Kaunas), 2022, 58(6): 745. |
| [8] | TOPOLNJAK R, SONKE J J, NIJKAMP J, et al. Breast patient setup error assessment: comparison of electronic portal image devices and cone-beam computed tomography matching results[J]. Int J Radiat Oncol Biol Phys, 2010, 78(4): 1235-1243. |
| [9] |
KEIPER T D, TAI A, CHEN X F, et al. Feasibility of real-time motion tracking using cine MRI during MR-guided radiation therapy for abdominal targets[J]. Med Phys, 2020, 47(8): 3554-3566.
doi: 10.1002/mp.14230 pmid: 32402111 |
| [10] | MALONE C, RYAN S, NICHOLSON J, et al. Intrafraction motion in surface-guided breast radiation therapy and its implications on a single planning target volume margin strategy[J]. Pract Radiat Oncol, 2025, 15(1): e63-e71. |
| [11] | TOKUDA P J K, MITSUYOSHI T, ONO Y, et al. Acute adverse events of ultra-hypofractionated whole-breast irradiation after breast-conserving surgery for early breast cancer in Japan: an interim analysis of the multi-institutional phase Ⅱ UPBEAT study[J]. Breast Cancer, 2024, 31(4): 643-648. |
| [12] |
LUO J R, YIN Z H, ZHANG Z, et al. Does the protocol-required uniform margin around the CTV adequately account for setup inaccuracies in whole breast irradiation?[J]. Radiat Oncol, 2021, 16(1): 143.
doi: 10.1186/s13014-021-01863-w pmid: 34344403 |
| [13] |
HOEKSTRA N, HABRAKEN S, SWAAK-KRAGTEN A, et al. Intrafraction motion during partial breast irradiation depends on treatment time[J]. Radiother Oncol, 2021, 159: 176-182.
doi: 10.1016/j.radonc.2021.03.029 pmid: 33798609 |
| [14] | BODA-HEGGEMANN J, KNOPF A C, SIMEONOVA-CHERGOU A, et al. Deep inspiration breath hold-based radiation therapy: a clinical review[J]. Int J Radiat Oncol Biol Phys, 2016, 94(3): 478-492. |
| [15] | HEIKKILÄ A, BOMAN E, ROSSI M, et al. Dosimetric effect of rotational setup errors in volumetric modulated arc therapy and field-in-field treatment of left-sided breast cancer[J]. Phys Med, 2024, 117: 103203. |
| [16] | LI G. Advances and potential of optical surface imaging in radiotherapy[J]. Phys Med Biol, 2022, 67(16): 10.1088/1361-10.1088/6560/ac838f. |
| [17] |
LIU H F, SCHAAL D, CURRY H, et al. Review of cone beam computed tomography based online adaptive radiotherapy: current trend and future direction[J]. Radiat Oncol, 2023, 18(1): 144.
doi: 10.1186/s13014-023-02340-2 pmid: 37660057 |
| [18] | RIETMAN J S, DIJKSTRA P U, GEERTZEN J B, et al. Treatment-related upper limb morbidity 1 year after sentinel lymph node biopsy or axillary lymph node dissection for stage Ⅰ or Ⅱ breast cancer[J]. Ann Surg Oncol, 2004, 11(11): 1018-1024. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd