欢迎访问《中国癌症杂志》官方网站,今天是
分享:
中国癌症杂志 ›› 2023, Vol. 33 ›› Issue (10): 936-944.doi: 10.19401/j.cnki.1007-3639.2023.10.006
赵博伦( ), 朱冠男()
), 朱冠男()
收稿日期:2023-05-16
修回日期:2023-10-01
出版日期:2023-10-30
发布日期:2023-10-31
通信作者:
朱冠男(ORCID: 0000-0002-2980-0074),博士,副主任医师,空军军医大学西京医院皮肤科主任。
作者简介:赵博伦(ORCID: 0000-0003-0326-459X),硕士研究生在读。
基金资助:
ZHAO Bolun(), ZHU Guannan()
Received:2023-05-16
Revised:2023-10-01
Published:2023-10-30
Online:2023-10-31
Contact:
ZHU Guannan.
文章分享
摘要:
黑色素瘤的发生、发展与多种癌基因的激活密切相关。15%~20%的黑色素瘤患者存在NRAS基因的激活突变,携带该突变基因的黑色素瘤具有更强的侵袭性,治疗难度大。由于RAS蛋白突变位点属于弱药物靶标,目前尚缺乏有效的靶向抑制剂,因此临床上多以免疫检查点抑制剂作为NRAS突变型晚期黑色素瘤的一线治疗方案,然而治疗反应率较低。近年来,在NRAS突变亚型中靶向治疗方案的探索主要集中在NRAS下游丝裂原活化蛋白激酶(mitogen-activated protein kinase,MAPK)通路,但结果不一:新型MEK1/2抑制剂tunlametinib,在晚期NRAS突变患者中总体客观缓解率(objective response rate,ORR)达到34.7%,较既往的binimetinib显著提高;然而泛RAF抑制剂belvarafenib和ERK抑制剂ulixertinib的Ⅰ期临床试验却未能展示出该药明显的优势。此外,以MEK抑制剂为基础的联合治疗也取得一定进展,现有证据表明,分子抑制剂类药物较免疫检查点抑制剂显示出更多的优势:选择性BRAF/CRAF抑制剂naporafenib(LXH254)与MEK抑制剂trametinib联合治疗NRAS突变型黑色素瘤的Ⅰb期临床试验中ORR达到46.7%;细胞周期蛋白依赖性激酶4/6(cyclin-dependent kinase4/6,CDK4/6)抑制剂ribociclib和binimetinib联合治疗在携带NRAS突变同时合并细胞周期蛋白基因异常的人群中可达32.5%;黏着斑激酶(focal adhesion kinase,FAK)抑制剂IN10018联合cobimetinib的研究结果也表现出较好的ORR(38.5%);但免疫检查点抑制剂程序性死亡[蛋白]配体-1(programmed death ligand-1,PD-L1)单抗durvalumab联合trametinib方案仅使27.2%的患者达到部分缓解(3/11)。与此同时,部分临床前研究结果也显示出一些转化潜质:如热激蛋白90(heat shock protein 90,HSP90)抑制剂XL888和丝氨酸/苏氨酸蛋白激酶19(serine/threonine protein kinase 19,STK19)抑制剂均在动物模型中表现出显著抑制NRAS突变型黑色素瘤细胞生长的能力。本文综述了NRAS突变型黑色素瘤的致癌机制及近年来治疗领域的研究进展,旨在展示该亚型患者的治疗现状,对多种新型治疗方法的临床研究结果进行总结和归纳,为当前临床实践和未来联合治疗方案提供依据。
中图分类号:
赵博伦, 朱冠男. NRAS突变型晚期黑色素瘤的治疗进展[J]. 中国癌症杂志, 2023, 33(10): 936-944.
ZHAO Bolun, ZHU Guannan. Advances in the treatment of advanced melanoma with NRAS gene mutation[J]. China Oncology, 2023, 33(10): 936-944.

图1
NRAS突变的信号转导示意图"
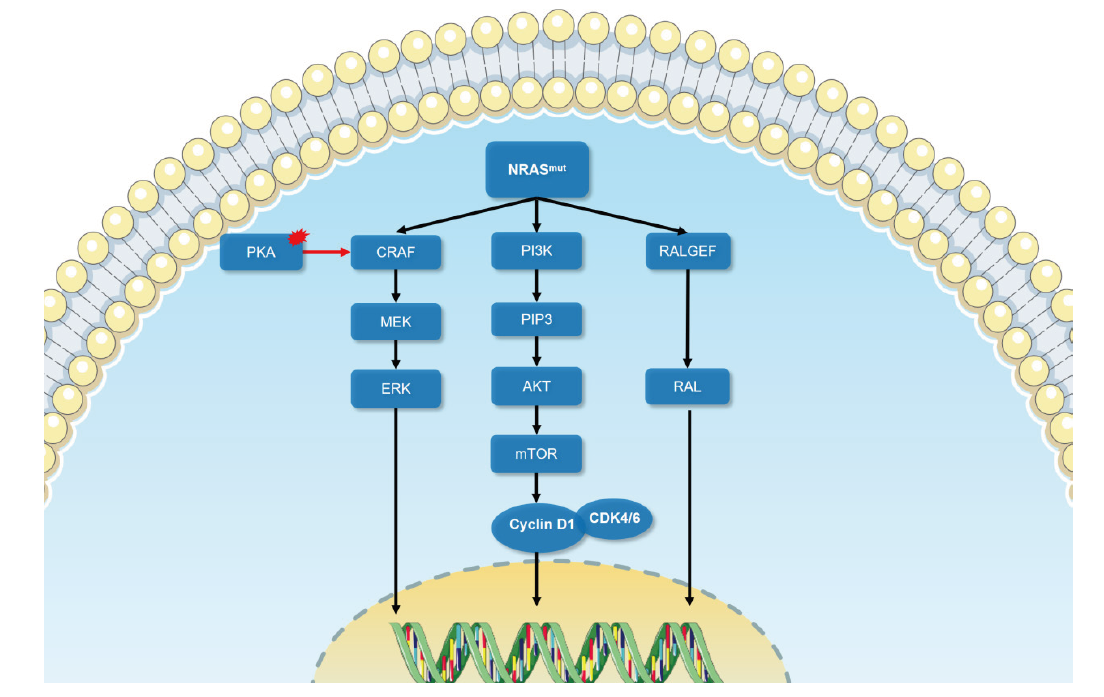
表1
针对NRAS突变型黑色素瘤的临床试验"
| Identifier | Target | Study design | NRAS-mutant mlanoma patients | Efficacy | Time frame |
|---|---|---|---|---|---|
| NCT03013101, NCT02821000, NCT02738489, CTR20160872[ | PD-1 antiboby | Clinical data from four clinical trials in patients with advanced melanoma treated with anti-PD-1 monoclonal antibodies between 2016 and 2019 were analyzed. The efficacy of immunotherapy in patients with cutaneous and non-cutaneous NRAS mutant melanoma was analyzed separately. | A total of 206 patients were assessed, including 12 patients with NRAS-mutated cutaneous melanoma and 21 patients with NRAS-mutated non-cutaneous melanoma | In cutaneous melanoma, patients with NRAS mutations had a lower overall response rate (ORR) than patients without NRAS mutations (9.5% vs 23.9%). In non-cutaneous melanoma, response rates were 0% and 13.7%, median progression-free survival (mPFS) was 3.6 months and 4.3 months (P=0.015), and median survival time (mOS) was 10.8 months and 15.3 months (P=0.025) in NRAS mutant and wild-type patients, respectively | 2016-2019 |
| NCT01763164[ | MEKi binimetinib | Phase Ⅲ randomized, multicenter, open-label clinical trial. Patients with advanced, unresectable stage ⅢC-Ⅳ NRAS mutated melanoma who were previously untreated or progressed following prior immunotherapy were randomized (2:1) to receive binimetinib 45 mg orally twice daily or dacarbazine 1 000 mg/m2 intravenously every 3 weeks. | A total of 402 patients with NRAS-mutated melanoma were enrolled, 269 treated with binimetinib and 233 treated with dacarbazine (1:2) | In the binimetinib arm mPFS was 2.8 months and 1.5 months in the dacarbazine arm | 2013-2015 |
| NCT01693068[ | MEKi pmasertib | Phase Ⅱ multicenter, open-label clinical trial. Patients with unresectable stage Ⅲc/ⅣM1 NRAS-mutated cutaneous melanoma were randomized 2:1 to receive pmasertib (60 mg orally twice daily) or DTIC (1 000 mg/m2 intravenously). Primary endpoint: investigator-assessed PFS; secondary endpoints: OS, ORR, quality of life (QoL), and safety. | 191 patients with NRAS mutated cutaneous melanoma, 191 treated (pimasertib n=130, DTIC n=61) | PFS and 6-month PFS rates were significantly improved in the pimasertib arm compared with the DTIC arm: 13 weeks versus 7 weeks, 17% vs 9%. Investigator-assessed ORR was 27% in the pimasertib arm and 14% in the DTIC arm. However, there was no difference in OS between patients treated with pimasertib and DTIC (mOS 9 and 11 months, respectively; HR=0.89, 95% CI: 0.61-1.30) | 2012-2014 |
| NCT00060125[ | Farnesyltransferase inhibitor (FTI) | Three-stage trial design, up to 40 patients, stopped early if first 14 patients did not respond, or first 28 patients had less than 2 responders | 14 patients with NRAS mutated melanoma | 2 patients presented with grade 3 toxicity and all patients had no clinical response and the trial was prematurely discontinued | 2003-2006 |
| Identifier | Target | Study design | NRAS-mutant mlanoma patients | Efficacy | Time frame |
| NCT03118817[ | RAFi belvarafenib | Single-arm, open-label, multicenter, phase Ⅰ extension study | 9 NRAS mutated melanoma patients | ORR 11%, mPFS 25 weeks | 2017-2020 |
| NCT03973151[ | MEKi HL-085 | Phase Ⅰ/Ⅱ, single-arm, dose-escalation and cohort expansion study | 42 patients with NRAS mutated melanoma | HL-085 was published in 2023 confirming an ORR of 34.7% | 2019-2023 |
| NCT02974725[ | BRAF/CRAF protein kinases inhibitor Naporafenib(LXH254) + MEKi trametinib | Phase Ⅰb escalation/expansion study | 30 patients with NRAS mutated melanoma | The ORR was 46.7%, the median DOR was 3.75 and the overall median PFS was 5.52 months in patients treated with naporafenib 200 mg twice a day plus trametinib 1 mg once daily. | 2017-2023 |
| NCT01449058[ | PI3Kαinhibitor BYL719 +MEKi binimetinib | Phase Ⅰb open-label, multicenter, dose escalation and expansion study | 5 NRAS mutated melanoma patients | ORR 20% | 2011-2017 |
| NCT01941927[ | MEKi trametinib +AKT inhibitor GSK2141795 | Phase Ⅱ non-randomized, multicenter, open-label clinical trial | Efficacy and safety of MEK inhibitors combined with AKT inhibitors in 10 patients with NRAS-mutated melanoma and 10 patients with BRAFWT/NRASWT melanoma | The mPFS and mOS of the 10 NRAS-mutated melanoma patients were only 2.3 and 4.0 months. Median PFS and OS for the wild-type cohort were 2.8 months and 3.5 months, respectively. No objective responses were identified in either cohort. The combination of Trametinib and GSK2141795 has no significant clinical activity in NRAS mutants or BRAFWT/NRASWT melanomas | 2013-2020 |
| NCT03932253 | MEKi FCN-159 | Phase Ⅰa/Ⅰb, open-label, dose escalation and dose expansion study | 33 patients with NRAS mutated melanoma were enrolled | The ORR and clinical benefit rates were 19.0% and 52.4%, respectively. Median duration of response and progression-free survival were 4.8 months and 3.8 months (1.8-5.6 months), respectively. | 2019-2023 |
| NCT03284502 | MEKi cobimetinib + RAFi HM95573 | Phase Ⅰb, open-label, multicenter dose escalation study | 9 NRAS mutated melanoma patients | Available data published ORR of 40% | 2017-2023 |
| NCT03979651 | MEKi trametinib+autophagy inhibitor hydroxychloroquine | Phase Ⅰb/Ⅱ non-randomized, open-label clinical trial | 29 NRAS mutated melanoma patients | Results to be further published | 2019-2022 |
| NCT04109456 | MEKi cobimetinib | Phase Ⅰb open-label clinical study | Estimated enrollment is 120 patients with NRAS mutated melanoma | Results to be further published | 2019-2023 |
| [1] |
TSAI F D, LOPES M S, ZHOU M, et al. KRAS4A splice variant is widely expressed in cancer and uses a hybrid membrane-targeting motif[J]. Proc Natl Acad Sci U S A, 2015, 112(3): 779-784.
doi: 10.1073/pnas.1412811112 |
| [2] |
MACARA I G. The ras superfamily of molecular switches[J]. Cell Signal, 1991, 3(3): 179-187.
pmid: 1892732 |
| [3] |
JAKOB J A, BASSETT R L Jr, NG C S, et al. NRAS mutation status is an independent prognostic factor in metastatic melanoma[J]. Cancer, 2012, 118(16): 4014-4023.
doi: 10.1002/cncr.26724 |
| [4] | 曾颖, 康晓静, 张祥月, 等. 肢端型黑素瘤NRAS基因突变检测及预后分析[J]. 中华皮肤科杂志, 2016, 49(7): 474-477. |
| [5] |
LALLY S E, MILMAN T, ORLOFF M, et al. Mutational landscape and outcomes of conjunctival melanoma in 101 patients[J]. Ophthalmology, 2022, 129(6): 679-693.
doi: 10.1016/j.ophtha.2022.01.016 |
| [6] |
LISZKAY G, MÁTRAI Z, CZIRBESZ K, et al. Predictive and prognostic value of BRAF and NRAS mutation of 159 sentinel lymph node cases in melanoma-a retrospective single-institute study[J]. Cancers (Basel), 2021, 13(13): 3302.
doi: 10.3390/cancers13133302 |
| [7] |
ZABLOCKA T, KREISMANE M, PJANOVA D, et al. Effects of BRAF V600E and NRAS mutational status on the progression-free survival and clinicopathological characteristics of patients with melanoma[J]. Oncol Lett, 2023, 25(1): 27.
doi: 10.3892/ol |
| [8] |
DUMAZ N, HAYWARD R, MARTIN J, et al. In melanoma, RAS mutations are accompanied by switching signaling from BRAF to CRAF and disrupted cyclic AMP signaling[J]. Cancer Res, 2006, 66(19): 9483-9491.
doi: 10.1158/0008-5472.CAN-05-4227 |
| [9] | PHADKE M S, SMALLEY K S M. Targeting NRAS mutations in advanced melanoma[J]. J Clin Oncol, 2023, 41(14): 2661-2664. |
| [10] |
SMALLEY K S, HAASS N K, BRAFFORD P A, et al. Multiple signaling pathways must be targeted to overcome drug resistance in cell lines derived from melanoma metastases[J]. Mol Cancer Ther, 2006, 5(5): 1136-1144.
pmid: 16731745 |
| [11] |
SHARMA A, TRIVEDI N R, ZIMMERMAN M A, et al. Mutant V599EB-Raf regulates growth and vascular development of malignant melanoma tumors[J]. Cancer Res, 2005, 65(6): 2412-2421.
doi: 10.1158/0008-5472.CAN-04-2423 |
| [12] | SATYAMOORTHY K, LI G, GERRERO M R, et al. Constitutive mitogen-activated protein kinase activation in melanoma is mediated by both BRAF mutations and autocrine growth factor stimulation[J]. Cancer Res, 2003, 63(4): 756-759. |
| [13] |
ZHUANG L, LEE C S, SCOLYER R A, et al. Activation of the extracellular signal regulated kinase (ERK) pathway in human melanoma[J]. J Clin Pathol, 2005, 58(11): 1163-1169.
doi: 10.1136/jcp.2005.025957 pmid: 16254105 |
| [14] |
OBA J, NAKAHARA T, ABE T, et al. Expression of c-Kit, p-ERK and cyclin D1 in malignant melanoma: an immunohistochemical study and analysis of prognostic value[J]. J Dermatol Sci, 2011, 62(2): 116-123.
doi: 10.1016/j.jdermsci.2011.02.011 pmid: 21454057 |
| [15] |
CANCER GENOME ATLAS NETWORK. Genomic classification of cutaneous melanoma[J]. Cell, 2015, 161(7): 1681-1696.
doi: 10.1016/j.cell.2015.05.044 pmid: 26091043 |
| [16] |
ROBERTSON G P. Functional and therapeutic significance of Akt deregulation in malignant melanoma[J]. Cancer Metastasis Rev, 2005, 24(2): 273-285.
doi: 10.1007/s10555-005-1577-9 |
| [17] |
XIE X Q, WHITE E P, MEHNERT J M. Coordinate autophagy and mTOR pathway inhibition enhances cell death in melanoma[J]. PLoS One, 2013, 8(1): e55096.
doi: 10.1371/journal.pone.0055096 |
| [18] |
ZIPFEL P A, BRADY D C, KASHATUS D F, et al. Ral activation promotes melanomagenesis[J]. Oncogene, 2010, 29(34): 4859-4864.
doi: 10.1038/onc.2010.224 pmid: 20562921 |
| [19] |
MISHRA P J, HA L, RIEKER J, et al. Dissection of RAS downstream pathways in melanomagenesis: a role for Ral in transformation[J]. Oncogene, 2010, 29(16): 2449-2456.
doi: 10.1038/onc.2009.521 |
| [20] |
FALSETTI S C, WANG D A, PENG H R, et al. Geranylgeranyltransferase Ⅰ inhibitors target RalB to inhibit anchorage-dependent growth and induce apoptosis and RalA to inhibit anchorage-independent growth[J]. Mol Cell Biol, 2007, 27(22): 8003-8014.
doi: 10.1128/MCB.00057-07 |
| [21] |
SINGHAL S S, AWASTHI Y C, AWASTHI S. Regression of melanoma in a murine model by RLIP76 depletion[J]. Cancer Res, 2006, 66(4): 2354-2360.
pmid: 16489041 |
| [22] | MARTÍN M T, ALCALDE M, PLOU F J, et al. Covalent immobilization of cyclodextrin glucosyltransferase (CGTase) in activated silica and Sepharose[J]. Indian J Biochem Biophys, 2002, 39(4): 229-234. |
| [23] |
SWETTER S M, THOMPSON J A, ALBERTINI M R, et al. NCCN guidelines® insights: melanoma: cutaneous, version 2.2021[J]. J Natl Compr Canc Netw, 2021, 19(4): 364-376.
doi: 10.6004/jnccn.2021.0018 |
| [24] |
MICHIELIN O, VAN AKKOOI A C J, ASCIERTO P A, et al. Cutaneous melanoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2019, 30(12): 1884-1901.
doi: S0923-7534(20)32563-1 pmid: 31987293 |
| [25] | JAEGER Z J, RAVAL N S, MAVERAKIS N K A, et al. Objective response to immune checkpoint inhibitor therapy in NRAS-mutant melanoma: a systematic review and meta-analysis[J]. Front Med (Lausanne), 2023, 10: 1090737. |
| [26] |
ZHOU L, WANG X, CHI Z H, et al. Association of NRAS mutation with clinical outcomes of anti-PD-1 monotherapy in advanced melanoma: a pooled analysis of four Asian clinical trials[J]. Front Immunol, 2021, 12: 691032.
doi: 10.3389/fimmu.2021.691032 |
| [27] |
DUMMER R, SCHADENDORF D, ASCIERTO P A, et al. Binimetinib versus dacarbazine in patients with advanced NRAS-mutant melanoma (NEMO): a multicentre, open-label, randomised, phase 3 trial[J]. Lancet Oncol, 2017, 18(4): 435-445.
doi: 10.1016/S1470-2045(17)30180-8 |
| [28] |
LEBBÉ C, DUTRIAUX C, LESIMPLE T, et al. Pimasertib versus dacarbazine in patients with unresectable NRAS-mutated cutaneous melanoma: phase Ⅱ, randomized, controlled trial with crossover[J]. Cancers (Basel), 2020, 12(7): 1727.
doi: 10.3390/cancers12071727 |
| [29] |
RYAN M B, CORCORAN R B. Therapeutic strategies to target RAS-mutant cancers[J]. Nat Rev Clin Oncol, 2018, 15(11): 709-720.
doi: 10.1038/s41571-018-0105-0 pmid: 30275515 |
| [30] |
GAJEWSKI T F, SALAMA A K S, NIEDZWIECKI D, et al. Phase Ⅱ study of the farnesyltransferase inhibitor R115777 in advanced melanoma (CALGB 500104)[J]. J Transl Med, 2012, 10: 246.
doi: 10.1186/1479-5876-10-246 |
| [31] |
FEDORENKO I V, GIBNEY G T, SMALLEY K M. NRAS mutant melanoma: biological behavior and future strategies for therapeutic management[J]. Oncogene, 2013, 32(25): 3009-3018.
doi: 10.1038/onc.2012.453 |
| [32] |
TATEISHI K, TSUBAKI M, TAKEDA T, et al. FTI-277 and GGTI-289 induce apoptosis via inhibition of the Ras/ERK and Ras/mTOR pathway in head and neck carcinoma HEp-2 and HSC-3 cells[J]. J BUON, 2021, 26(2): 606-612.
pmid: 34077012 |
| [33] |
SKOULIDIS F, LI B T, DY G K, et al. Sotorasib for lung cancers with KRAS p.G12C mutation[J]. N Engl J Med, 2021, 384(25): 2371-2381.
doi: 10.1056/NEJMoa2103695 |
| [34] |
HONG D S, FAKIH M G, STRICKLER J H, et al. KRASG12C inhibition with sotorasib in advanced solid tumors[J]. N Engl J Med, 2020, 383(13): 1207-1217.
doi: 10.1056/NEJMoa1917239 |
| [35] |
JAISWAL B S, JANAKIRAMAN V, KLJAVIN N M, et al. Combined targeting of BRAF and CRAF or BRAF and PI3K effector pathways is required for efficacy in NRAS mutant tumors[J]. PLoS One, 2009, 4(5): e5717.
doi: 10.1371/journal.pone.0005717 |
| [36] |
YEN I, SHANAHAN F, LEE J, et al. ARAF mutations confer resistance to the RAF inhibitor belvarafenib in melanoma[J]. Nature, 2021, 594(7863): 418-423.
doi: 10.1038/s41586-021-03515-1 |
| [37] |
WANG X, LUO Z G, CHEN J, et al. First-in-human phase I dose-escalation and dose-expansion trial of the selective MEK inhibitor HL-085 in patients with advanced melanoma harboring NRAS mutations[J]. BMC Med, 2023, 21(1): 2.
doi: 10.1186/s12916-022-02669-7 |
| [38] |
ADAM C, FUSI L, WEISS N, et al. Efficient suppression of NRAS-driven melanoma by Co-inhibition of ERK1/2 and ERK5 MAPK pathways[J]. J Invest Dermatol, 2020, 140(12): 2455-2465.e10.
doi: 10.1016/j.jid.2020.03.972 |
| [39] |
CARLINO M S, TODD J R, GOWRISHANKAR K, et al. Differential activity of MEK and ERK inhibitors in BRAF inhibitor resistant melanoma[J]. Mol Oncol, 2014, 8(3): 544-554.
doi: 10.1016/j.molonc.2014.01.003 |
| [40] |
MENDZELEVSKI B, FERBER G, JANKU F, et al. Effect of ulixertinib, a novel ERK1/2 inhibitor, on the QT/QTc interval in patients with advanced solid tumor malignancies[J]. Cancer Chemother Pharmacol, 2018, 81(6): 1129-1141.
doi: 10.1007/s00280-018-3564-1 |
| [41] |
ATEFI M, TITZ B, AVRAMIS E, et al. Combination of pan-RAF and MEK inhibitors in NRAS mutant melanoma[J]. Mol Cancer, 2015, 14(1): 27.
doi: 10.1186/s12943-015-0293-5 |
| [42] | DE BRAUD F, DOOMS C, HEIST R S, et al. Initial evidence for the efficacy of naporafenib in combination with trametinib in NRAS-mutant melanoma: results from the expansion arm of a phase ib, open-label study[J]. J Clin Oncol, 2023, 41(14): 2651-2660. |
| [43] |
POSCH C, MOSLEHI H, FEENEY L, et al. Combined targeting of MEK and PI3K/mTOR effector pathways is necessary to effectively inhibit NRAS mutant melanoma in vitro and in vivo[J]. Proc Natl Acad Sci U S A, 2013, 110(10): 4015-4020.
doi: 10.1073/pnas.1216013110 |
| [44] |
JURIC D, SORIA J C, SHARMA S, et al. A phase 1b dose-escalation study of BYL719 plus binimetinib (MEK162) in patients with selected advanced solid tumors[J]. J Clin Oncol, 2014, 32(15_suppl): 9051.
doi: 10.1200/jco.2014.32.15_suppl.9051 |
| [45] | ALGAZI A P, ESTEVE-PUIG R, NOSRATI A, et al. Dual MEK/AKT inhibition with trametinib and GSK2141795 does not yield clinical benefit in metastatic NRAS-mutant and wild-type melanoma[J]. Pigment Cell Melanoma Res, 2018, 31(1): 110-114. |
| [46] |
SCHULER M, ZIMMER L, KIM K B, et al. Phase Ⅰb/Ⅱ trial of ribociclib in combination with binimetinib in patients with NRAS-mutant melanoma[J]. Clin Cancer Res, 2022, 28(14): 3002-3010.
doi: 10.1158/1078-0432.CCR-21-3872 |
| [47] | InxMed releases data demonstrating IN10018 therapeutic potential in patients with metastatic melanoma at SMR 2022[R]. SMR, October 17-20, 2022 (Abstract:141). |
| [48] |
KINSEY C G, CAMOLOTTO S A, BOESPFLUG A M, et al. Protective autophagy elicited by RAF→MEK→ERK inhibition suggests a treatment strategy for RAS-driven cancers[J]. Nat Med, 2019, 25(4): 620-627.
doi: 10.1038/s41591-019-0367-9 |
| [49] |
RIBAS A, ALGAZI A, ASCIERTO P A, et al. PD-L1 blockade in combination with inhibition of MAPK oncogenic signaling in patients with advanced melanoma[J]. Nat Commun, 2020, 11(1): 6262.
doi: 10.1038/s41467-020-19810-w pmid: 33288749 |
| [50] |
GOGAS H, DRÉNO B, LARKIN J, et al. Cobimetinib plus atezolizumab in BRAFV600 wild-type melanoma: primary results from the randomized phase Ⅲ IMspire170 study[J]. Ann Oncol, 2021, 32(3): 384-394.
doi: 10.1016/j.annonc.2020.12.004 |
| [51] | GAO X J, XUE D D, CHENG J J, et al. Inhibition of axl promotes the therapeutic effect of targeted inhibition of the PI3K/Akt pathway in NRAS mutant melanoma cells[J]. J Oncol, 2022, 2022: 2946929. |
| [52] |
LI S, WU X, YAN X, et al. Toripalimab plus axitinib in patients with metastatic mucosal melanoma: 3-year survival update and biomarker analysis[J]. J Immunother Cancer, 2022, 10(2): e004036.
doi: 10.1136/jitc-2021-004036 |
| [53] |
PUZANOV I, SOSMAN J, SANTORO A, et al. Phase Ⅰ trial of tivantinib in combination with sorafenib in adult patients with advanced solid tumors[J]. Invest New Drugs, 2015, 33(1): 159-168.
doi: 10.1007/s10637-014-0167-5 |
| [54] |
MAO L, GUO J, ZHU L, et al. A first-in-human, phase 1a dose-escalation study of the selective MEK1/2 inhibitor FCN-159 in patients with advanced NRAS-mutant melanoma[J]. Eur J Cancer, 2022, 175: 125-135.
doi: 10.1016/j.ejca.2022.08.005 |
| [55] |
HAARBERG H E, PARAISO K H, WOOD E, et al. Inhibition of Wee1, AKT, and CDK4 underlies the efficacy of the HSP90 inhibitor XL888 in an in vivo model of NRAS-mutant melanoma[J]. Mol Cancer Ther, 2013, 12(6): 901-912.
doi: 10.1158/1535-7163.MCT-12-1003 |
| [56] |
QIAN L, CHEN K, WANG C H, et al. Targeting NRAS-mutant cancers with the selective STK19 kinase inhibitor chelidonine[J]. Clin Cancer Res, 2020, 26(13): 3408-3419.
doi: 10.1158/1078-0432.CCR-19-2604 |
| [1] | 冯欣滢, 王冰, 刘培峰. 腹膜转移癌腹腔化疗的创新与挑战[J]. 中国癌症杂志, 2024, 34(9): 827-837. |
| [2] | 曹晓珊, 杨蓓蓓, 丛斌斌, 刘红. 三阴性乳腺癌脑转移治疗的研究进展[J]. 中国癌症杂志, 2024, 34(8): 777-784. |
| [3] | 黄思捷, 康勋, 李文斌. 鞘内注射治疗实体瘤脑膜转移的临床研究进展[J]. 中国癌症杂志, 2024, 34(7): 695-701. |
| [4] | 李晓辉, 赵加旭, 彭海豹, 张叶, 曾睿, 迟喻丹. HMGA2对软脑膜转移黑色素瘤细胞迁移和增殖的影响[J]. 中国癌症杂志, 2024, 34(4): 389-399. |
| [5] | 许永虎, 徐大志. 21世纪以来胃癌治疗进展及未来展望[J]. 中国癌症杂志, 2024, 34(3): 239-249. |
| [6] | 陈亦凡, 李婷, 王碧芸. CCR8在肿瘤免疫治疗中的研究进展[J]. 中国癌症杂志, 2024, 34(3): 299-305. |
| [7] | 金奕滋, 林明曦, 曾铖, 郭晴, 张剑. 雌激素受体低表达早期乳腺癌的研究进展[J]. 中国癌症杂志, 2024, 34(10): 972-978. |
| [8] | 刘雪柔, 杨玉梅, 赵倩, 荣翔宇, 刘伟, 郑瑞洁, 庞金龙, 李娴, 李姗姗. 谷氨酰胺代谢相关蛋白在肿瘤转移中的作用研究进展[J]. 中国癌症杂志, 2024, 34(1): 97-103. |
| [9] | 康殷楠, 陈顺, 解有成, 郑英, 何昱静, 李初谊, 于晓辉. 抗体药物偶联物在HER2阳性晚期胃癌中的应用进展和展望[J]. 中国癌症杂志, 2023, 33(8): 790-800. |
| [10] | 吴晶, 周娟, 苏春霞. 肺癌脂肪酸代谢重编程的研究进展[J]. 中国癌症杂志, 2023, 33(5): 517-526. |
| [11] | 蒋金玲, 周尘飞, 王超, 赵丽琴, 吴珺玮, 张俊. 2022年度胃癌研究和诊疗新进展[J]. 中国癌症杂志, 2023, 33(4): 303-314. |
| [12] | 杨梓怡, 李盼丽, 顾丙新, 刘成, 宋少莉, 许晓平. 68Ga-DOTA-PDL1P的设计合成及其在黑色素瘤小鼠模型中的应用研究[J]. 中国癌症杂志, 2023, 33(4): 354-360. |
| [13] | 田熙, 徐文浩, 朱殊璇, 艾合太木江·安外尔, 宿佳琦, 叶世琪, 瞿元元, 施国海, 张海梁, 叶定伟. 2022年度肾细胞癌基础研究及临床诊疗新进展[J]. 中国癌症杂志, 2023, 33(3): 191-200. |
| [14] | 苏春霞, 周彩存. 2022年度肺癌领域重要临床研究进展[J]. 中国癌症杂志, 2023, 33(3): 218-227. |
| [15] | 曹晓珊, 丛斌斌. 三阳性乳腺癌内分泌治疗联合靶向治疗的研究进展[J]. 中国癌症杂志, 2023, 33(3): 288-292. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
地址:上海市徐汇区东安路270号复旦大学附属肿瘤医院10号楼415室
邮编:200032 电话:021-64188274 E-mail:zgazzz@china-oncology.com
访问总数:; 今日访问总数:; 当前在线人数:
本系统由北京玛格泰克科技发展有限公司设计开发 技术支持:support@magtech.com.cn