欢迎访问《中国癌症杂志》官方网站,今天是
分享:
中国癌症杂志 ›› 2022, Vol. 32 ›› Issue (3): 274-286.doi: 10.19401/j.cnki.1007-3639.2022.03.011
• 指南与共识 • 上一篇
中国抗癌协会乳腺癌专业委员会, 长江学术带乳腺联盟
收稿日期:2022-01-17
修回日期:2022-01-25
出版日期:2022-03-30
发布日期:2022-04-02
通信作者:
长江学术带乳腺联盟
The Society of Breast Cancer of China Anti-Cancer Association, Breast Cancer Study Group Along Yangtze River
Received:2022-01-17
Revised:2022-01-25
Published:2022-03-30
Online:2022-04-02
Contact:
Breast Cancer Study Group Along Yangtze River
文章分享
摘要:
早期乳腺癌女性患者的骨健康管理包括骨丢失的管理和骨转移的预防。随着早期乳腺癌患者生存期不断延长,这些患者的骨健康问题受到广泛关注,但目前临床上尚无系统的管理方案及诊疗措施。因此,中国抗癌协会乳腺癌专业委员会和长江学术带乳腺联盟组织相关专家,基于国内外指南及循证医学证据,深入探讨并制定了《早期乳腺癌女性患者的骨健康管理中国专家共识(2022年版)》,希望通过本共识规范早期乳腺癌患者的骨健康管理。
中图分类号:
中国抗癌协会乳腺癌专业委员会, 长江学术带乳腺联盟. 早期乳腺癌女性患者的骨健康管理中国专家共识(2022年版)[J]. 中国癌症杂志, 2022, 32(3): 274-286.
The Society of Breast Cancer of China Anti-Cancer Association, Breast Cancer Study Group Along Yangtze River. Chinese expert consensus recommendations for management of bone health in female patients with early breast cancer (2022 edition)[J]. China Oncology, 2022, 32(3): 274-286.
图1
骨健康管理推荐路径 a:抗肿瘤治疗前已经发生的骨丢失可视为non-CTIBL。b:见表1。c:43%的专家认为患者骨折风险分级中危时即可给予骨改良药物干预。d:年龄>65岁、T值<-1.5、现在吸烟及有吸烟史、BMI<24、髋骨骨折家族史、50岁以上脆性骨折个人史、口服糖皮质激素>6个月。e:若防治骨丢失与预防骨转移有冲突,以干预方式强和用药频率高的方式为准。BMI:体重指数(body mass index)。"
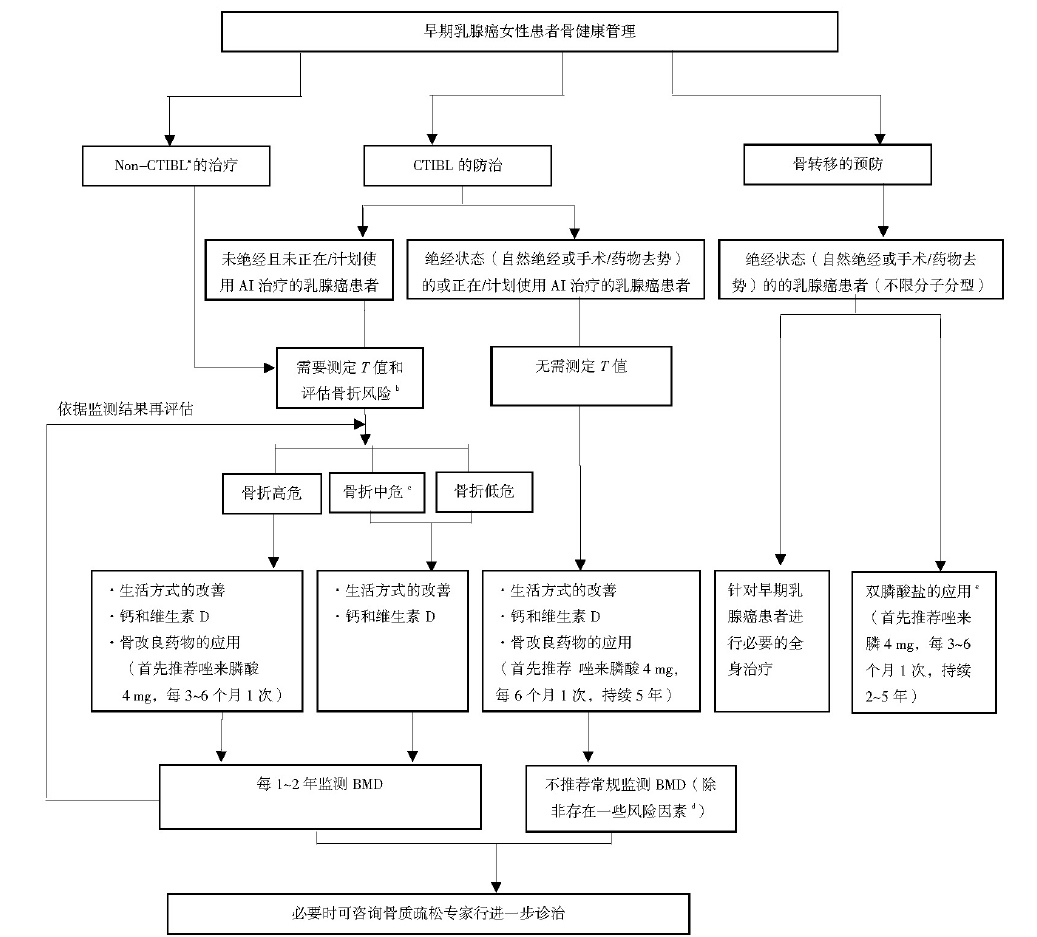
表1
CTIBL导致骨折的风险分级"
| 风险分级 | 风险分级影响因素 |
|---|---|
| 低危 | T值≥-1.0 |
| 中危 | -2.0<T值<-1.0 |
| 高危 | T值≤-2.0,或-2.0<T值<-1.0同时存在任意两个 风险因素(年龄>65岁、T值<-1.5、现在吸烟及有吸烟史、BMI<24、髋骨骨折家族史、 50岁以上脆性骨折个人史、口服糖皮质激素 >6个月) |
表2
骨改良药物对乳腺癌患者BMD的影响"
| 研究名称 | 研究类型 | 入组人群 | 治疗方案 | 骨改良药物干预时机 | 治疗时间/年 | 结论 |
|---|---|---|---|---|---|---|
| ABCSG-12研究 [ | 随机、开放Ⅲ期临床试验 | 1 800例绝经前HR+早期乳腺癌患者 | 内分泌治疗+唑来膦酸(4 mg/6个月) vs 内分泌治疗 | 内分泌治疗的同时立即接受唑来膦酸治疗 | 3 | ① 内分泌治疗(OFS+AI/TAM)会引起严重的骨丢失(-13.6%,平均差为-0.141 g/cm,95% CI:-0.179~-0.102 vs -9.0%,平均差为-0.95 g/cm,95% CI:-0.134~-0.570,P<0.000 1),且OFS+AI治疗引起的骨丢失更严重;② 唑来膦酸联合内分泌治疗(OFS+TAM/AI)可有效防止内分泌治疗带来的骨丢失(+0.4%,平均差为0.004 g/ cm,95% CI:-0.024~0.032),并且治疗结束后2年对患者的BMD仍有改善(4.0%,平均差为0.039 g/cm2,95% CI:0.005~0.075,P=0.02) |
| HOBOE研究 [ | 多中心、随机、对照Ⅲ期临床试验 | 483例HR+早期乳腺癌患者 | 绝经前:OFS + TAM vs OFS+AI vs OFS+AI+唑来膦酸(4 mg/6个月);绝经后:TAM vs AI vs AI +唑来膦酸(4 mg/6个月) | 内分泌治疗的同时立即接受唑来膦酸治疗 | 5 | ① 联合唑来膦酸组(AI+唑来膦酸)比非联合唑来膦酸组(AI)BMD得到有效改善(0.60,95% CI:0.46~0.77,P<0.000 1),并且绝经前与绝经后患者结果相似;② 内分泌治疗(AI/OFS+AI)会引起骨丢失,而唑来膦酸可预防内分泌治疗引起的骨丢失 |
| ARIBON研究 [ | 双盲、随机、安慰剂对照Ⅲ期临床研究 | 131例绝经后ER+早期乳腺癌患者 | AI+口服伊班膦酸(150 mg/个月) vs AI+安慰剂 | 内分泌治疗的同时接受口服伊班膦酸治疗 | 5 | 2年后,口服伊班膦酸组椎骨和髋关节BMD分别增加2.98%(-8.9~19.9)和0.60%(-9.0~6.9),安慰剂组腰椎BMD降低3.22%(-16.0~4.3),髋关节BMD降低3.90%(-12.3~7.2)。两个治疗组在两个部位的差异均有统计学意义(P<0.01)。根据治疗2年后的BMD情况,T值<-2.5的患者继续接受口服伊班膦酸治疗直至5年。5年后,口服伊班膦酸组椎骨BMD增加9.65%,髋关节BMD增加2.72% |
| ABCSG-18研究 [ | 随机、双盲、安慰剂对照Ⅲ期临床研究 | 3 420例绝经后早期HR+乳腺癌患者 | AI+地舒单抗(60 mg/6个月) vs AI + 安慰剂 | 内分泌治疗的同时接受地舒单抗治疗 | 3 | ① AI联合地舒单抗组首次发生骨折的临床时间明显延迟(风险比为0.50,95% CI:0.39~0.65,P<0.000 1);② AI联合地舒单抗组骨折总数低于安慰剂组,无论是基线T值≥-1亚组(风险比为0.44,95% CI:0.31~0.64,P<0.000 1)还是基线T值<-1亚组(风险比为0.57,95% CI:0.40~0.82,P=0.002) |
| HALT-BC研究 [ | 随机、双盲、安慰剂对照Ⅲ期临床试验 | 252例HR+乳腺癌患者 | AI+地舒单抗(60 mg/6个月) vs AI + 安慰剂 | 内分泌治疗的同时接受地舒单抗治疗 | 2 | 12和24个月时,地舒单抗组与安慰剂组相比腰椎BMD分别增加了5.5%(P<0.001)和7.6%(P<0.001) |
表3
双膦酸盐对早期乳腺癌患者生存获益的影响"
| 研究名称 | 研究类型 | 入组人群 | 治疗方案 | 双膦酸盐干预时机 | 治疗时 间/年 | 中位随访时间 | DFS | OS |
|---|---|---|---|---|---|---|---|---|
| ABCSG-12研究 [ | 随机、开放Ⅲ期临床试验 | 1 800例绝经前HR+早期乳腺癌患者 | OFS+TAM/AI+唑来膦(4 mg/6个月)vs OFS+TAM/AI | 内分泌治疗的同时立即接受唑来膦酸治疗 | 3 | 94.4个月 | 联合唑来膦酸组与单独内分泌治疗相比,DFS率增长3.4%(88.4% vs 85.0%),复发风险降低23%(风险比为0.77,95% CI:0.60~0.99,P=0.042) | 联合唑来膦酸组与无唑来膦酸组相比OS率更高(96.7% vs 94.5%),死亡风险绝对值降低2.2% |
| HOBOE2研究 [ | 多中心、随机、对照Ⅲ期临床试验 | 1 065例绝经前HR+早期乳腺癌患者 | OFS+TAM vs OFS+AI vs OFS + AI+唑来膦酸(4 mg/6个月) | 内分泌治疗的同时立即接受唑来膦酸治疗 | 治疗5年或治疗至患者55岁 | 64.0个月 | OFS+TAM的5年DFS率为96.9%,OFS+AI的5年DFS率为98.4%,OFS+AI+唑来膦酸的5年DFS率为99.7%(P=0.008);OFS+AI+唑来膦酸 vs OFS+TAM:风险比为0.52(95% CI:0.34~0.80,P=0.003);OFS+AI+唑来膦酸 vs OFS+AI:风险比为0.70(95% CI:0.44~1.12,P=0.22) | OFS+TAM的5年OS率为96.9%(95% CI:94.1~98.4),OFS+AI的5年OS率为98.4%(95% CI:96.2~99.3),OFS+AI+唑来膦酸的5年OS率为99.7%(95% CI:97.9~100.0) |
| AZURE研究 [ | 多中心、随机、开放、平行对照Ⅲ期临床试验 | 3 360例女性乳腺癌患者(HR+、HER2+、三阴性) | 系统治疗# vs 系统治疗+唑来膦酸(4 mg/6个月) | 系统治疗的同时立即接受唑来膦酸治疗 | 5 | 117.0个月 | ① 绝经后患者:系统治疗联合唑来膦酸可降低18%的疾病复发风险(风险比为0.82,95% CI:0.67~1.00),降低22%的侵袭性疾病发生风险(风险比为0.78,95% CI:0.64~0.94);② MAF基因*阴性(拷贝数<2.5)的患者:系统治疗联合唑来膦酸可降低25%的侵袭性疾病发生风险(风险比为0.75,95% CI:0.58~0.97,P=0.026) | MAF基因阴性(拷贝数<2.5)的患者:系统治疗联合唑来膦酸可降低31%的死亡风险(风险比为0.69,95% CI:0.50~0.94,P=0.019) |
| SUCCESS A试验 [ | 多中心、随机、开放Ⅲ期临床试验 | 3 754例有淋巴结阳性或高风险淋巴结阴性(以下至少1种:肿瘤大小≥pT2,组织学分级3级,HR阴性,年龄≤35岁)的原发性浸润性乳腺癌患者 | 化疗后,患者分别接受5年唑来膦酸治疗(4 mg/3个月,持续2年,随后4 mg/6个月,持续3年)和2年唑来膦酸治疗(4 mg/3个月,持续2年) | 患者接受6个周期的化疗后,立即接受唑来膦酸治疗 | 5 vs 2 | 唑来膦酸治疗2年后开始测量生存时间 | 5年DFS率 vs 2年DFS率:风险比为0.97(95% CI:0.75~1.25,P=0.81) 5年无远处转移生存率 vs 2年无远处转移生存率:风险比为0.87(95% CI:0.65~1.18,P=0.38) | 风险比为0.98,95% CI:0.67~1.42,P=0.90 |
| EBCTCG/meta分析 [ | 纳入26项随机、对照临床试验 | 18 766例早期HR+乳腺癌患者(其中使用唑来膦酸的患者有9 290例) | 内分泌治疗方案 vs 内分泌治疗方案+双膦酸盐 | 内分泌治疗的同时立即接受双膦酸盐治疗 | / | / | 联合双膦酸盐在降低绝经后患者疾病复发率(风险比为0.86,95% CI:0.78~0.94,P=0.002 0)、远处复发率(风险比为0.82,95% CI:0.74~0.92,P=0.000 3)和骨转移发生率(风险比为0.72,95% CI:0.60~0.86,P=0.000 2)方面均有获益; | 联合双膦酸盐在降低绝经后患者死亡率(风险比为0.82,95% CI:0.73~0.93,P=0.002 0)方面有明显获益 |
| Meta分析1 [ | 纳入8项随机对照研究 | 7 730例早期HR+乳腺癌患者 | 内分泌治疗方案 vs 内分泌治疗方案+唑来膦酸 | 内分泌治疗的同时立即接受唑来膦酸治疗 | / | / | 联合唑来膦酸可使患者的5年DFS率有改善趋势(RR=0.90,95% CI:0.81~1.00,P=0.06) | 联合唑来膦酸可使患者的5年OS率显著改善(RR=0.86,95% CI:0.75~0.99,P=0.03) |
| Meta分析2 [ | 纳入7项随机对照研究 | 3 969例早期HR+乳腺癌患者 | 内分泌治疗方案 vs 内分泌治疗方案+唑来膦酸 | 内分泌治疗的同时立即接受唑来膦酸治疗 | / | / | 联合唑来膦酸治疗使患者的DFS有改善趋势(风险比为0.75,95% CI:0.52~1.08,P=0.121) | 联合唑来膦酸治疗可显著延长乳腺癌患者的OS(风险比为0.85,95% CI:0.73~1.00,P=0.047) |
表4
地舒单抗对早期乳腺癌患者生存获益的影响"
| 研究名称 | 研究类型 | 入组人群 | 治疗方案 | 地舒单抗干预时机 | 治疗时 间/年 | 中位随访时间 | DFS | OS |
|---|---|---|---|---|---|---|---|---|
| ABCSG-18研究 [ | 多中心、前瞻性、双盲、安慰剂对照Ⅲ期临床试验 | 3 425例绝经后早期HR+乳腺癌患者 | AI+地舒单抗(60 mg/6个月) vs AI+安慰剂 | 内分泌治疗的同时接受地舒单抗治疗 | 3 | 73个月 | 地舒单抗组的DFS率显著提高(风险比为0.82,95% CI:0.69~0.98,多因素比例风险回归模型分析,P=0.026 0;描述性统计学分析,未控制多重性);地舒单抗组的5年DFS率为89.2%(95% CI:87.6~90.8),8年DFS率为80.6%(95% CI:78.1~83.1),而安慰剂组5年DFS率为87.3%(95% CI:85.7~89.0),8年DFS率为77.5%(95% CI:74.8-80.2) | / |
| D-CARE研究 [ | 国际、双盲、随机、安慰剂对照Ⅲ期临床试验 | 4 509例乳腺癌患者(HR+、HER2+) | 系统治疗+安慰剂 vs 系统治疗+地舒单抗(120 mg/3~4周,持续6个月,120 mg/12周) | 新辅助和辅助化疗的同时接受地舒单抗治疗 | 5 | 67个月 | ① 无骨转移生存率:地舒单抗组与安慰剂组无明显差异(风险比为0.97,95% CI:0.82~1.14,P=0.70),各亚组中两组均无差异均无统计学意义;② DFS:地舒单抗组与安慰剂组无明显差异(风险比为1.04,95% CI:0.91~1.19,P=0.57),各亚组中差异均无统计学意义 | / |
| [1] | FERLAY J, COLOMBET M, SOERJOMATARAM I, et al. Cancer statistics for the year 2020: an overview[J]. Int J Cancer, 2021. [Online ahead of print] |
| [2] | HOWLADER N, ALTEKRUSE S F, LI C I, et al. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status[J]. J Natl Cancer Inst, 2014, 106(5): dju055. |
| [3] | RIZZOLI R, BISCHOFF-FERRARI H, DAWSON-HUGHES B, et al. Nutrition and bone health in women after the menopause[J]. Womens Health (Lond), 2014, 10(6): 599-608. |
| [4] |
DIANA A N, CARLINO F, GIUNTA E F, et al. Cancer treatment-induced bone loss (CTIBL): state of the art and proper management in breast cancer patients on endocrine therapy[J]. Curr Treat Options Oncol, 2021, 22(5): 45.
doi: 10.1007/s11864-021-00835-2 |
| [5] |
RACHNER T D, COLEMAN R, HADJI P, et al. Bone health during endocrine therapy for cancer[J]. Lancet Diabetes Endocrinol, 2018, 6(11): 901-910.
doi: 10.1016/S2213-8587(18)30047-0 |
| [6] |
LEE Y K, LEE E G, KIM H Y, et al. Osteoporotic fractures of the spine, hip, and other locations after adjuvant endocrine therapy with aromatase inhibitors in breast cancer patients: a meta-analysis[J]. J Korean Med Sci, 2020, 35(46): e403.
doi: 10.3346/jkms.2020.35.e403 |
| [7] |
BODY J J. Increased fracture rate in women with breast cancer: a review of the hidden risk[J]. BMC Cancer, 2011, 11: 384.
doi: 10.1186/1471-2407-11-384 |
| [8] | CLYNES M A, HARVEY N C, CURTIS E M, et al. The epidemiology of osteoporosis[J]. Br Med Bull, 2020, 133(1): 105-117. |
| [9] | RASHKI KEMMAK A, REZAPOUR A, JAHANGIRI R, et al. Economic burden of osteoporosis in the world: a systematic review[J]. Med J Islam Repub Iran, 2020, 34: 154. |
| [10] |
KEY T, APPLEBY P, BARNES I, et al. Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies[J]. J Natl Cancer Inst, 2002, 94(8): 606-616.
doi: 10.1093/jnci/94.8.606 |
| [11] |
FRANCIS P A, PAGANI O, FLEMING G F, et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer[J]. N Engl J Med, 2018, 379(2): 122-137.
doi: 10.1056/NEJMoa1803164 |
| [12] |
CUZICK J, SESTAK I, BAUM M, et al. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial[J]. Lancet Oncol, 2010, 11(12): 1135-1141.
doi: 10.1016/S1470-2045(10)70257-6 |
| [13] |
REGAN M M, NEVEN P, GIOBBIE-HURDER A, et al. Assessment of letrozole and tamoxifen alone and in sequence for postmenopausal women with steroid hormone receptor-positive breast cancer: the BIG 1-98 randomised clinical trial at 8.1 years median follow-up[J]. Lancet Oncol, 2011, 12(12): 1101-1108.
doi: 10.1016/S1470-2045(11)70270-4 |
| [14] |
NICKS K M, FOWLER T W, AKEL N S, et al. Bone turnover across the menopause transition: the role of gonadal inhibins[J]. Ann N Y Acad Sci, 2010, 1192: 153-160.
doi: 10.1111/j.1749-6632.2009.05349.x |
| [15] |
FOGELMAN I, BLAKE G M, BLAMEY R, et al. Bone mineral density in premenopausal women treated for node-positive early breast cancer with 2 years of goserelin or 6 months of cyclophosphamide, methotrexate and 5-fluorouracil (CMF)[J]. Osteoporos Int, 2003, 14(12): 1001-1006.
doi: 10.1007/s00198-003-1508-y |
| [16] |
HADJI P, ZILLER M, KIEBACK D G, et al. Effects of exemestane and tamoxifen on bone health within the tamoxifen exemestane adjuvant multicentre (TEAM) trial: results of a German, 12-month, prospective, randomised substudy[J]. Ann Oncol, 2009, 20(7): 1203-1209.
doi: 10.1093/annonc/mdn762 |
| [17] |
HADJI P, GNANT M, BODY J J, et al. Cancer treatment-induced bone loss in premenopausal women: a need for therapeutic intervention?[J]. Cancer Treat Rev, 2012, 38(6): 798-806.
doi: 10.1016/j.ctrv.2012.02.008 |
| [18] |
NUZZO F, GALLO C, LASTORIA S, et al. Bone effect of adjuvant tamoxifen, letrozole or letrozole plus zoledronic acid in early-stage breast cancer: the randomized phase 3 HOBOE study[J]. Ann Oncol, 2012, 23(8): 2027-2033.
doi: 10.1093/annonc/mdr600 |
| [19] | BURSTEIN H J, LACCHETTI C, ANDERSON H, et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update[J]. J Clin Oncol, 2019, 37(5): 423-438. |
| [20] | 马远征, 王以朋, 刘强, 等. 中国老年骨质疏松诊疗指南(2018)[J]. 中国老年学杂志, 2019, 39(11): 2557-2575. |
| MA Y Z, WANG Y P, LIU Q, et al. 2018 China guideline for the diagnosis and treatment of senile osteoporosis[J]. Chin J Gerontol, 2019, 39(11): 2557-2575. | |
| [21] |
COLEMAN R, HADJI P, BODY J J, et al. Bone health in cancer: ESMO clinical practice guidelines[J]. Ann Oncol, 2020, 31(12): 1650-1663.
doi: 10.1016/j.annonc.2020.07.019 |
| [22] | 中国抗癌协会乳腺癌专业委员会. 中国抗癌协会乳腺癌诊治指南与规范(2021年版)[J]. 中国癌症杂志, 2021, 31(10): 954-1040. |
| The Society of Breast Cancer China Anti-Cancer Association. Guidelines for breast cancer diagnosis and treatment by China Anti-Cancer Association (2021 edition)[J]. China Oncol, 2021, 31(10): 954-1040. | |
| [23] |
HANDFORTH C, D'ORONZO S, COLEMAN R, et al. Cancer treatment and bone health[J]. Calcif Tissue Int, 2018, 102(2): 251-264.
doi: 10.1007/s00223-017-0369-x |
| [24] |
WEAVER C M, ALEXANDER D D, BOUSHEY C J, et al. Calcium plus vitamin D supplementation and risk of fractures: an updated meta-analysis from the National Osteoporosis Foundation[J]. Osteoporos Int, 2016, 27(1): 367-376.
doi: 10.1007/s00198-015-3386-5 |
| [25] |
HADJI P, AAPRO M S, BODY J J, et al. Management of aromatase inhibitor-associated bone loss in postmenopausal women with breast cancer: practical guidance for prevention and treatment[J]. Ann Oncol, 2011, 22(12): 2546-2555.
doi: 10.1093/annonc/mdr017 |
| [26] |
中华医学会骨质疏松和骨矿盐疾病分会. 原发性骨质疏松症诊疗指南(2017)[J]. 中国全科医学, 2017, 20(32): 3963-3982.
doi: 10.3969/j.issn.1007-9572.2017.00.118 |
| Chinese Society of Osteoporosis and Bone Mineral Research. Guidelines for the diagnosis and treatment of primary osteoporosis (2017)[J]. Chin Gen Pract, 2017, 20(32): 3963-3982. | |
| [27] | 邵志敏, 沈镇宙, 徐兵河. 乳腺肿瘤学[M]. 上海: 复旦大学出版社, 2013. |
| SHAO Z M, SHEN Z Z, XU B H. Breast oncology[M]. Shanghai: Fudan University Press, 2013. | |
| [28] | MEI M, XIANG Z, YANG J, et al. Efficacy of zoledronic acid for prevention of bone loss in early-stage breast cancer patients receiving adjuvant therapy: a meta-analysis of 13 randomized controlled trials[J]. Curr Probl Cancer, 2020, 44(2): 100507. |
| [29] | 中国医师协会肿瘤医师分会乳腺癌学组, 中国抗癌协会国际医疗交流分会. 骨改良药物安全性管理专家共识[J]. 中华肿瘤杂志, 2021, 43(6): 622-628. |
| Breast Cancer Division, Oncologist Branch of Chinese Medical Association; International Medical Exchange Branch of Chinese Anti-Cancer Association. Expert consensus on safety management of bone-modifying agents[J]. Chin J Oncol, 2021, 43(6): 622-628. | |
| [30] |
VEHMANEN L K, ELOMAA I, BLOMQVIST C P, et al. The effect of ovarian dysfunction on bone mineral density in breast cancer patients 10 years after adjuvant chemotherapy[J]. Acta Oncol, 2014, 53(1): 75-79.
doi: 10.3109/0284186X.2013.792992 |
| [31] |
GNANT M F X, MLINERITSCH B, LUSCHIN-EBENGREUTH G, et al. Zoledronic acid prevents cancer treatment-induced bone loss in premenopausal women receiving adjuvant endocrine therapy for hormone-responsive breast cancer: a report from the Austrian Breast and Colorectal Cancer Study Group[J]. J Clin Oncol, 2007, 25(7): 820-828.
doi: 10.1200/JCO.2005.02.7102 |
| [32] |
GNANT M, MLINERITSCH B, LUSCHIN-EBENGREUTH G, et al. Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 5-year follow-up of the ABCSG-12 bone-mineral density substudy[J]. Lancet Oncol, 2008, 9(9): 840-849.
doi: 10.1016/S1470-2045(08)70204-3 |
| [33] |
LESTER J E, DODWELL D, PUROHIT O P, et al. Prevention of anastrozole-induced bone loss with monthly oral ibandronate during adjuvant aromatase inhibitor therapy for breast cancer[J]. Clin Cancer Res, 2008, 14(19): 6336-6342.
doi: 10.1158/1078-0432.CCR-07-5101 |
| [34] |
LESTER J E, DODWELL D, BROWN J E, et al. Prevention of anastrozole induced bone loss with monthly oral ibandronate: final 5 year results from the ARIBON trial[J]. J Bone Oncol, 2012, 1(2): 57-62.
doi: 10.1016/j.jbo.2012.06.002 |
| [35] |
GNANT M, PFEILER G, DUBSKY P C, et al. Adjuvant denosumab in breast cancer (ABCSG-18): a multicentre, randomised, double-blind, placebo-controlled trial[J]. Lancet, 2015, 386(9992): 433-443.
doi: 10.1016/S0140-6736(15)60995-3 |
| [36] |
ELLIS G K, BONE H G, CHLEBOWSKI R, et al. Randomized trial of denosumab in patients receiving adjuvant aromatase inhibitors for nonmetastatic breast cancer[J]. J Clin Oncol, 2008, 26(30): 4875-4882.
doi: 10.1200/JCO.2008.16.3832 |
| [37] |
SHAPIRO C L, VAN POZNAK C, LACCHETTI C, et al. Management of osteoporosis in survivors of adult cancers with nonmetastatic disease: ASCO clinical practice guideline[J]. J Clin Oncol, 2019, 37(31): 2916-2946.
doi: 10.1200/JCO.19.01696 |
| [38] | NCCN clinical practice guidelines in oncology (breast cancer) (version 5.2021)[EB/OL]. [2021-06-28]. http://www.nccn.org/patients. |
| [39] |
BUNDRED N J, CAMPBELL I D, DAVIDSON N, et al. Effective inhibition of aromatase inhibitor-associated bone loss by zoledronic acid in postmenopausal women with early breast cancer receiving adjuvant letrozole: ZO-FAST study results[J]. Cancer, 2008, 112(5): 1001-1010.
doi: 10.1002/(ISSN)1097-0142 |
| [40] |
EIDTMANN H, DE BOER R, BUNDRED N, et al. Efficacy of zoledronic acid in postmenopausal women with early breast cancer receiving adjuvant letrozole: 36-month results of the ZO-FAST study[J]. Ann Oncol, 2010, 21(11): 2188-2194.
doi: 10.1093/annonc/mdq217 |
| [41] |
COLEMAN R, DE BOER R, EIDTMANN H, et al. Zoledronic acid (zoledronate) for postmenopausal women with early breast cancer receiving adjuvant letrozole (ZO-FAST study): final 60-month results[J]. Ann Oncol, 2013, 24(2): 398-405.
doi: 10.1093/annonc/mds277 |
| [42] |
DERENNE S, AMIOT M, BARILLÉ S, et al. Zoledronate is a potent inhibitor of myeloma cell growth and secretion of IL-6 and MMP-1 by the tumoral environment[J]. J Bone Miner Res, 1999, 14(12): 2048-2056.
doi: 10.1359/jbmr.1999.14.12.2048 |
| [43] |
APARICIO A, GARDNER A, TU Y, et al. In vitro cytoreductive effects on multiple myeloma cells induced by bisphosphonates[J]. Leukemia, 1998, 12(2): 220-229.
doi: 10.1038/sj.leu.2400892 |
| [44] |
FROMIGUE O, LAGNEAUX L, BODY J J. Bisphosphonates induce breast cancer cell death in vitro[J]. J Bone Miner Res, 2000, 15(11): 2211-2221.
doi: 10.1359/jbmr.2000.15.11.2211 |
| [45] |
SENARATNE S G, PIRIANOV G, MANSI J L, et al. Bisphosphonates induce apoptosis in human breast cancer cell lines[J]. Br J Cancer, 2000, 82(8): 1459-1468.
doi: 10.1054/bjoc.1999.1131 |
| [46] | BOISSIER S, FERRERAS M, PEYRUCHAUD O, et al. Bisphosphonates inhibit breast and prostate carcinoma cell invasion, an early event in the formation of bone metastases[J]. Cancer Res, 2000, 60(11): 2949-2954. |
| [47] |
WOOD J, BONJEAN K, RUETZ S, et al. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid[J]. J Pharmacol Exp Ther, 2002, 302(3): 1055-1061.
doi: 10.1124/jpet.102.035295 |
| [48] |
COLEMAN R, WOODWARD E, BROWN J, et al. Safety of zoledronic acid and incidence of osteonecrosis of the jaw (ONJ) during adjuvant therapy in a randomised phase Ⅲ trial (AZURE: BIG 01-04) for women with stage Ⅱ/Ⅲ breast cancer[J]. Breast Cancer Res Treat, 2011, 127(2): 429-438.
doi: 10.1007/s10549-011-1429-y |
| [49] |
COLEMAN R, CAMERON D, DODWELL D, et al. Adjuvant zoledronic acid in patients with early breast cancer: final efficacy analysis of the AZURE (BIG 01/04) randomised open-label phase 3 trial[J]. Lancet Oncol, 2014, 15(9): 997-1006.
doi: 10.1016/S1470-2045(14)70302-X |
| [50] |
COLEMAN R, HALL A, ALBANELL J, et al. Effect of MAF amplification on treatment outcomes with adjuvant zoledronic acid in early breast cancer: a secondary analysis of the international, open-label, randomised, controlled, phase 3 AZURE (BIG 01/04) trial[J]. Lancet Oncol, 2017, 18(11): 1543-1552.
doi: 10.1016/S1470-2045(17)30603-4 |
| [51] |
COLEMAN R E, COLLINSON M, GREGORY W, et al. Benefits and risks of adjuvant treatment with zoledronic acid in stage Ⅱ/Ⅲ breast cancer. 10 years follow-up of the AZURE randomized clinical trial (BIG 01/04)[J]. J Bone Oncol, 2018, 13: 123-135.
doi: 10.1016/j.jbo.2018.09.008 |
| [52] |
GNANT M, MLINERITSCH B, STOEGER H, et al. Zoledronic acid combined with adjuvant endocrine therapy of tamoxifen versus anastrozol plus ovarian function suppression in premenopausal early breast cancer: final analysis of the Austrian Breast and Colorectal Cancer Study Group trial 12[J]. Ann Oncol, 2015, 26(2): 313-320.
doi: 10.1093/annonc/mdu544 |
| [53] |
PERRONE F, DE LAURENTIIS M, DE PLACIDO S, et al. Adjuvant zoledronic acid and letrozole plus ovarian function suppression in premenopausal breast cancer: HOBOE phase 3 randomised trial[J]. Eur J Cancer, 2019, 118: 178-186.
doi: 10.1016/j.ejca.2019.05.004 |
| [54] |
FRIEDL T W P, FEHM T, MÜLLER V, et al. Prognosis of patients with early breast cancer receiving 5 years vs 2 years of adjuvant bisphosphonate treatment: a phase 3 randomized clinical trial[J]. JAMA Oncol, 2021, 7(8): 1149-1157.
doi: 10.1001/jamaoncol.2021.1854 |
| [55] |
Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Adjuvant bisphosphonate treatment in early breast cancer: meta-analyses of individual patient data from randomised trials[J]. Lancet, 2015, 386(10001): 1353-1361.
doi: 10.1016/S0140-6736(15)60908-4 |
| [56] |
HE M F, FAN W D, ZHANG X Q. Adjuvant zoledronic acid therapy for patients with early stage breast cancer: an updated systematic review and meta-analysis[J]. J Hematol Oncol, 2013, 6(1): 80.
doi: 10.1186/1756-8722-6-80 |
| [57] |
HUANG W W, HUANG C, LIU J, et al. Zoledronic acid as an adjuvant therapy in patients with breast cancer: a systematic review and meta-analysis[J]. PLoS One, 2012, 7(7): e40783.
doi: 10.1371/journal.pone.0040783 |
| [58] |
GNANT M, PFEILER G, STEGER G G, et al. Adjuvant denosumab in postmenopausal patients with hormone receptor-positive breast cancer (ABCSG-18): disease-free survival results from a randomised, double-blind, placebo-controlled, phase 3 trial[J]. Lancet Oncol, 2019, 20(3): 339-351.
doi: 10.1016/S1470-2045(18)30862-3 |
| [59] |
COLEMAN R, FINKELSTEIN D M, BARRIOS C, et al. Adjuvant denosumab in early breast cancer (D-CARE): an international, multicentre, randomised, controlled, phase 3 trial[J]. Lancet Oncol, 2020, 21(1): 60-72.
doi: 10.1016/S1470-2045(19)30687-4 |
| [60] | EISEN A, SOMERFIELD M R, ACCORDINO M K, et al. Use of adjuvant bisphosphonates and other bone-modifying agents in breast cancer: ASCO-OH (CCO) guideline update[J]. J Clin Oncol, 2022. [Online ahead of print] |
| [61] | GREGORY W, MARSHALL H, BELL R, et al. Adjuvant zoledronic acid (ZOL) in postmenopausal women with breast cancer and those rendered postmenopausal: results of a meta-analysis[J]. J Clin Oncol, 2012, 30(15_suppl): 513. |
| [1] | 徐睿, 王泽浩, 吴炅. 肿瘤相关中性粒细胞在乳腺癌发生、发展中的作用研究进展[J]. 中国癌症杂志, 2024, 34(9): 881-889. |
| [2] | 曹晓珊, 杨蓓蓓, 丛斌斌, 刘红. 三阴性乳腺癌脑转移治疗的研究进展[J]. 中国癌症杂志, 2024, 34(8): 777-784. |
| [3] | 张剑. 关于女性乳腺癌患者绝经状态判断两个关键问题的临床思考[J]. 中国癌症杂志, 2024, 34(7): 619-627. |
| [4] | 姜丹, 宋国庆, 王晓丹. 乳腺癌中线粒体功能障碍与CPT1A/ERK信号转导通路共同调节乳腺癌恶性行为的机制研究[J]. 中国癌症杂志, 2024, 34(7): 650-658. |
| [5] | 董涧桥, 李坤艳, 李菁, 王斌, 王艳红, 贾红燕. SIRT3通过去乙酰化YME1L1诱导乳腺癌内分泌治疗耐药的作用机制研究[J]. 中国癌症杂志, 2024, 34(6): 537-547. |
| [6] | 郝弦, 黄建军, 杨文秀, 刘晋廷, 张军红, 罗钰蓓, 李青, 王大红, 高玉炜, 谭福云, 薄莉, 郑羽, 王荣, 冯江龙, 李静, 赵春华, 豆晓伟. 乳腺癌原代细胞系为药物筛选和基础研究提供癌症新模型[J]. 中国癌症杂志, 2024, 34(6): 561-570. |
| [7] | 中国抗癌协会乳腺癌专业委员会. 中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)[J]. 中国癌症杂志, 2024, 34(3): 316-333. |
| [8] | 张琪, 修秉虬, 吴炅. 2023年中国乳腺癌重要临床研究成果及最新进展[J]. 中国癌症杂志, 2024, 34(2): 135-142. |
| [9] | 张思源, 江泽飞. 2023年改变晚期乳腺癌临床实践的重要研究成果及进展[J]. 中国癌症杂志, 2024, 34(2): 143-150. |
| [10] | 王昭卜, 黎星, 于鑫淼, 金锋. 2023年改变早期乳腺癌临床实践的重要研究成果及进展[J]. 中国癌症杂志, 2024, 34(2): 151-160. |
| [11] | 罗扬, 孙涛, 邵志敏, 崔久嵬, 潘跃银, 张清媛, 程颖, 李惠平, 杨燕, 叶长生, 于国华, 王京芬, 刘运江, 刘新兰, 周宇红, 柏玉举, 谷元廷, 王晓稼, 徐兵河, 宋礼华. AK-HER2与参照药治疗HER2阳性转移性乳腺癌患者的疗效、体内代谢特征、安全性和免疫原性比较:一项多中心、随机、双盲Ⅲ期等效性临床试验[J]. 中国癌症杂志, 2024, 34(2): 161-175. |
| [12] | 陈远香, 余涛, 杨诗雨, 曾涛, 魏兰, 张彦. KDM4A通过下调BMP9促进乳腺癌细胞MDA-MB-231的迁移和侵袭[J]. 中国癌症杂志, 2024, 34(2): 176-184. |
| [13] | 胡晓钰, 蔡毓文, 叶富贵, 邵志敏, 胡伟刚, 余科达. BRCA1/2胚系突变对三阴性乳腺癌患者放疗后第二原发肿瘤的影响[J]. 中国癌症杂志, 2024, 34(2): 185-190. |
| [14] | 张思维, 马丁, 江一舟, 邵志敏. 聚力分型精准,引领诊疗变革——乳腺癌精准诊疗新模式[J]. 中国癌症杂志, 2024, 34(11): 1045-1052. |
| [15] | 欧阳飞, 王阳, 陈瑜, 裴国清, 王陵, 张扬, 石磊. 基于机器学习构建乳腺癌骨转移预测模型[J]. 中国癌症杂志, 2024, 34(10): 903-914. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||
地址:上海市徐汇区东安路270号复旦大学附属肿瘤医院10号楼415室
邮编:200032 电话:021-64188274 E-mail:zgazzz@china-oncology.com
访问总数:; 今日访问总数:; 当前在线人数:
本系统由北京玛格泰克科技发展有限公司设计开发 技术支持:support@magtech.com.cn