Welcome to China Oncology,
China Oncology ›› 2022, Vol. 32 ›› Issue (3): 251-257.doi: 10.19401/j.cnki.1007-3639.2022.03.008
• Article • Previous Articles Next Articles
TANG Bo( ), ZHAO Xia, LIU Hongbing, ZHANG Qingfeng, LIU Kui
), ZHAO Xia, LIU Hongbing, ZHANG Qingfeng, LIU Kui
Received:2021-11-19
Revised:2022-02-22
Online:2022-03-30
Published:2022-04-02
Contact:
TANG Bo
E-mail:dskdfo_3002@163.com
Share article
CLC Number:
TANG Bo, ZHAO Xia, LIU Hongbing, ZHANG Qingfeng, LIU Kui. Application of end-to-end double-layer hand-sewn esophagogastric anastomosis and gastric fundus embedding during minimally invasive esophagectomy for esophageal cancer[J]. China Oncology, 2022, 32(3): 251-257.
Tab. 1
Clinicopathological characteristics of 129 patients with esophageal carcinoma"
| Characteristic | End-to-end anastomosis group (N=87) | End-to-side anastomosis group (N=42) | t value | P value |
|---|---|---|---|---|
| Age/year $\bar{x}±s$ | 64.0±11.5 | 63.0±12.8 | 0.74 | 0.461 |
| Gender | 0.129 | 0.493 | ||
| Male | 68 | 34 | ||
| Female | 19 | 8 | ||
| Body mass index $\bar{x}±s$ | 24.8±3.9 | 25.3±4.2 | 0.349 | 0.754 |
| TNM stage of tumor | 0.069 | 0.815 | ||
| Ⅱ | 18 | 8 | ||
| Ⅲ | 58 | 27 | ||
| Ⅳa | 11 | 7 | ||
| Chemotherapy/radiotherapy | 4.351 | 0.037 | ||
| Yes | 11 | 1 | ||
| No | 76 | 41 | ||
| Cardiovascular | 0.759 | 0.384 | ||
| Yes | 8 | 6 | ||
| No | 79 | 36 | ||
| Diabetes | 0.014 | 0.995 | ||
| Yes | 11 | 5 | ||
| No | 76 | 37 | ||
| Chronic obstructive pulmonary disease | 0.799 | 0.371 | ||
| Yes | 15 | 4 | ||
| No | 72 | 38 |
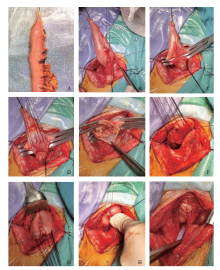
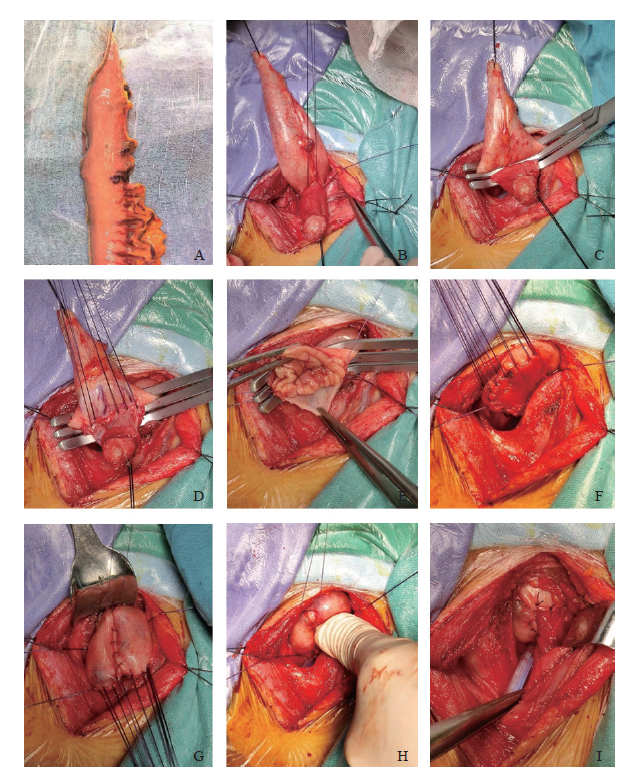
Fig. 1
end-to-end double-layer esophagogastric anastomosis and gastric fundus embedding A: The small curvature of the stomach was resected with a cutting suture device to make a conical tubular stomach. B: Use 4-0 silk thread to fix the posterior wall of esophagus and stomach with 4 stitches. C: Place trefoil forceps. D: The muscular layer of esophagus and stomach was incised, the muscular layer was sutured intermittently, and the first layer of the posterior wall was anastomosed. E: The mucosal layers of the esophagus and stomach are sutured continuously. F: The esophagus and the muscularis of the anterior wall of the stomach were sutured intermittently and the trefoil forceps were withdrawn. G: The anterior wall of stomach was sutured with a needle. H: The stoma is stuffed into the stomach. I: The esophagus and stomach were fixed with 3 needles to complete the suture of anterior wall."
Tab. 2
Operative and perioperative data of 129 patients with esophageal carcinoma"
| Data | End-to-end anastomosis group (N=87) | End-to-side anastomosis group (N=42) | t value | P value |
|---|---|---|---|---|
| Operative time t/min $\bar{x}±s$ | 248±32 | 224±36 | 0.523 | 0.603 |
| Time for anastomosis t/min $\bar{x}±s$ | 32.0±6.8 | 15.0±5.4 | 3.576 | 0.021 |
| Blood loss V/mL $\bar{x}±s$ | 115±46 | 105±35 | 0.750 | 0.528 |
| Postoperative day t/d $\bar{x}±s$ | 11.2±2.0 | 14.4±5.8 | 1.764 | 0.112 |
| Anastomotic leakage n | 1 | 5 | 5.162 | 0.023 |
| Anastomotic stricture n | 13 | 8 | 0.350 | 0.554 |
| Gastroesophageal reflux n | 8 | 11 | 6.514 | 0.011 |
| Other postoperative complication n | ||||
| Vocal cord paralysis | 10 | 4 | 0.001 | 0.972 |
| Thoracic gastric dilatation | 1 | 0 | 0.687 | 0.484 |
| Arrhythmia | 9 | 11 | 5.429 | 0.020 |
| Pneumonia | 11 | 13 | 6.270 | 0.012 |
| Chylothorax | 1 | 1 | 0.281 | 0.547 |
| [1] |
YUAN Y, WANG K N, CHEN L Q. Esophageal anastomosis[J]. Dis Esophagus, 2015, 28(2): 127-137.
doi: 10.1111/dote.2015.28.issue-2 |
| [2] | 王海军, 韩泳涛. 食管癌术后吻合口瘘诊治进展[J]. 临床外科杂志, 2016, 24(7): 543-545. |
| WANG H J, HAN Y T. Progress in diagnosis and treatment of anastomotic fistula after esophageal carcinoma[J]. J Clin Surg, 2016, 24(7): 543-545. | |
| [3] | 毛友生, 高树庚, 王群, 等. 中国食管癌临床流行特征及外科治疗概况大数据分析[J]. 中华肿瘤杂志, 2020, 42(3): 228-233. |
| MAO Y S, GAO S G, WANG Q, et al. Epidemiological characteristic and current status of surgical treatment for esophageal cancer by analysis of national registry database[J]. Chin J Oncol, 2020, 42(3): 228-233. | |
| [4] |
HONDA M, KURIYAMA A, NOMA H, et al. Hand-sewn versus mechanical esophagogastric anastomosis after esophagectomy: a systematic review and meta-analysis[J]. Ann Surg, 2013, 257(2): 238-248.
doi: 10.1097/SLA.0b013e31826d4723 |
| [5] | YUAN Y, ZENG X X, HU Y, et al. AOmentoplasty for oesophagogastrostomy after oesophagectomy[J]. Cochrane Database Syst Rev, 2014(10): CD008446. |
| [6] |
LERUT T, COOSEMANS W, DECKER G, et al. Anastomotic complications after esophagectomy[J]. Dig Surg, 2002, 19(2): 92-98.
doi: 10.1159/000052018 |
| [7] |
XU Q R, WANG K N, WANG W P, et al. Linear stapled esophagogastrostomy is more effective than hand-sewn or circular stapler in prevention of anastomotic stricture: a comparative clinical study[J]. J Gastrointest Surg, 2011, 15(6): 915-921.
doi: 10.1007/s11605-011-1490-1 |
| [8] |
WANG W P, GAO Q, WANG K N, et al. A prospective randomized controlled trial of semi-mechanical versus hand-sewn or circular stapled esophagogastrostomy for prevention of anastomotic stricture[J]. World J Surg, 2013, 37(5): 1043-1050.
doi: 10.1007/s00268-013-1932-x |
| [9] | 陈传贵, 于振涛, 金庆文, 等. 食管癌术后吻合口瘘的临床特点及危险因素分析[J]. 中华外科杂志, 2015, 53(7): 518-521. |
| CHEN C G, YU Z T, JIN Q W, et al. Clinical features and risk factors of anastomotic leakage after radical esophagectomy[J]. Chin J Surg, 2015, 53(7): 518-521. | |
| [10] | GOENSE L, VAN ROSSUM P S, TROMP M, et al. Intraoperative and postoperative risk factors for anastomotic leakage and pneumonia after esophagectomy for cancer[J]. Dis Esophagus, 2017, 30(1): 1-10. |
| [11] |
KASSIS E S, KOSINSKI A S, ROSS P Jr, et al. Predictors of anastomotic leak after esophagectomy: an analysis of the society of thoracic surgeons general thoracic database[J]. Ann Thorac Surg, 2013, 96(6): 1919-1926.
doi: 10.1016/j.athoracsur.2013.07.119 |
| [12] | 聂洪鑫, 王兵, 杨思豪, 等. 食管癌术后食管胃吻合口瘘危险因素的系统评价与Meta分析[J]. 中国胸心血管外科临床杂志, 2022, 29(2): 166-178. |
| NIE H X, WANG B, YANG S H, et al. Risk factors for esophagogastric anastomotic leakage after esophageal cancer surgery: a systematic review and meta-analysis[J]. Chin J Clin Thorac Cardiovasc Surg, 2022, 29(2): 166-178. | |
| [13] | 张灿斌, 李简, 郑建, 等. 胃管成形术在食管重建中的可行性研究[J]. 河南科技大学学报(医学版), 2005, 23(3): 175-179. |
| ZHANG C B, LI J, ZHENG J, et al. Feasible study for construction of gastric tube in esophageal reconstruction[J]. J Henan Univ Sci Technol Medicial Sci, 2005, 23(3): 175-179. | |
| [14] |
VAN WORKUM F, VAN DER MAAS J, VAN DEN WILDENBERG F J, et al. Improved functional results after minimally invasive esophagectomy: intrathoracic versus cervical anastomosis[J]. Ann Thorac Surg, 2017, 103(1): 267-273.
doi: 10.1016/j.athoracsur.2016.07.010 |
| [15] |
KUMAGAI K, ROUVELAS I, TSAI J A, et al. Meta-analysis of postoperative morbidity and perioperative mortality in patients receiving neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal and gastro-oesophageal junctional cancers[J]. Br J Surg, 2014, 101(4): 321-338.
doi: 10.1002/bjs.9418 |
| [16] |
ROH S, IANNETTONI M D, KEECH J, et al. Timing of esophagectomy after neoadjuvant chemoradiation therapy affects the incidence of anastomotic leaks[J]. Korean J Thorac Cardiovasc Surg, 2019, 52(1): 1-8.
doi: 10.5090/kjtcs.2019.52.1.1 |
| [17] |
MARKAR S R, KARTHIKESALINGAM A, VYAS S, et al. Hand-sewn versus stapled oesophago-gastric anastomosis: systematic review and meta-analysis[J]. J Gastrointest Surg, 2011, 15(5): 876-884.
doi: 10.1007/s11605-011-1426-9 |
| [18] |
YUAN Y, ZENG X X, ZHAO Y F, et al. Modified double-layer anastomosis for minimally invasive esophagectomy: an effective way to prevent leakage and stricture[J]. World J Surg, 2017, 41(12): 3164-3170.
doi: 10.1007/s00268-017-4126-0 |
| [19] |
CORSINI E M, HOFSTETTER W L, et al. Ketorolac use and anastomotic leak in patients with esophageal cancer[J]. J Thorac Cardiovasc Surg, 2021, 161(2): 448-454.
doi: 10.1016/j.jtcvs.2020.02.133 |
| [20] |
VAN DER SCHAAF M, JOHAR A, LAGERGREN P, et al. Surgical prevention of reflux after esophagectomy for cancer[J]. Ann Surg Oncol, 2013, 20(11): 3655-3661.
doi: 10.1245/s10434-013-3041-3 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd