Welcome to China Oncology,
China Oncology ›› 2023, Vol. 33 ›› Issue (4): 361-367.doi: 10.19401/j.cnki.1007-3639.2023.04.006
• Article • Previous Articles Next Articles
BI Zhao( ), CHEN Peng, QIU Pengfei, CHEN Yuguang, WANG Yongsheng()
), CHEN Peng, QIU Pengfei, CHEN Yuguang, WANG Yongsheng()
Received:2022-12-05
Revised:2023-03-24
Online:2023-04-30
Published:2023-05-15
Contact:
WANG Yongsheng
Share article
CLC Number:
BI Zhao, CHEN Peng, QIU Pengfei, CHEN Yuguang, WANG Yongsheng. The analysis of axillary lymph nodes metastasis after neoadjuvant therapy in breast cancer[J]. China Oncology, 2023, 33(4): 361-367.
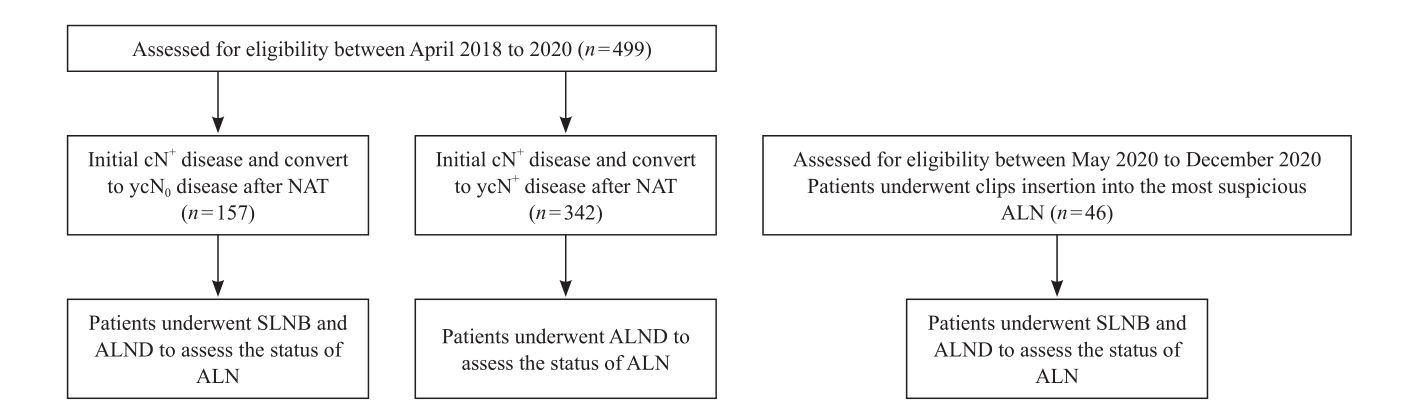
Fig. 1
The flow chart of study"
Tab. 1
The clinical characteristics of 499 patients"
| Characteristics | Patients n (%) |
|---|---|
| Molecular subtypes | |
| HER2+ | 219 (43.9) |
| TNBC | 204 (40.9) |
| HR+/HER2- | 76 (15.2) |
| Clinical nodal stage | |
| cN1 | 305 (61.1) |
| cN2 | 130 (26.1) |
| cN3 | 64 (12.8) |
| Clinical tumor stage | |
| cT1 | 44 (8.9) |
| cT2 | 254 (50.9) |
| cT3 | 83 (16.6) |
| cT4 | 118 (23.6) |
| Axillary surgery | |
| SLNB+ALND | 157 (31.5) |
| ALND | 342 (68.5) |
Tab. 2
The distribution of ALN at different levels in SLN-positive group after NAT"
| SLN+ | Status of ALN at different levels | Patients n (%) | ||
|---|---|---|---|---|
| L1 | L2 | L3 | ||
| cN1 group | - | - | - | 23 (67.6) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 6 (17.6) | |
| + | - | + | 1 (3.0) | |
| + | + | - | 3 (8.8) | |
| + | + | + | 1 (3.0) | |
| cN2 group | - | - | - | 9 (50.0) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 5 (27.7) | |
| + | - | + | 1 (5.6) | |
| + | + | - | 1 (5.6) | |
| + | + | + | 2 (11.1) | |
| cN3 group | - | - | - | 2 (33.2) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 1 (16.7) | |
| + | - | - | 1 (16.7) | |
| + | - | + | 1 (16.7) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 1 (16.7) | |
Tab. 3
The distribution of ALN at different levels in SLN-negative group after NAT"
| SLN- | Status of ALN at different levels | Patients n (%) | ||
|---|---|---|---|---|
| L1 | L2 | L3 | ||
| cN1 group | - | - | - | 57 (91.9) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 4 (6.5) | |
| + | - | + | 0 (0.0) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 1 (1.6) | |
| cN2 group | - | - | - | 21 (91.3) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 2 (8.7) | |
| + | - | + | 0 (0.0) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 0 (0.0) | |
| cN3 group | - | - | - | 111 (78.7) |
| - | + | + | 1 (7.1) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 1 (7.1) | |
| + | - | + | 0 (0.0) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 1 (7.1) | |
Tab. 4
The analysis of ALN distribution and number of negative SLNs after NAT"
| Negative SLN | Status of ALN at different levels | Patients n (%) | ||
|---|---|---|---|---|
| L1 | L2 | L3 | ||
| 1 SLN- | - | - | - | 30 (88.2) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 3 (8.8) | |
| + | - | + | 0 (0.0) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 1 (3.0) | |
| 2 SLN- | - | - | - | 21 (95.5) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 1 (4.5) | |
| + | - | + | 0 (0.0) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 0 (0.0) | |
| 3 SLN- | - | - | - | 6 (100.0) |
| - | + | + | 0 (0.0) | |
| - | - | + | 0 (0.0) | |
| - | + | - | 0 (0.0) | |
| + | - | - | 0 (0.0) | |
| + | - | + | 0 (0.0) | |
| + | + | - | 0 (0.0) | |
| + | + | + | 0 (0.0) | |
| [1] |
《中国乳腺癌新辅助治疗专家共识2022年版》专家组. 中国乳腺癌新辅助治疗专家共识(2022年版)[J]. 中国癌症杂志, 2022, 32(1): 80-89.
doi: 10.19401/j.cnki.1007-3639.2022.01.011 |
| Expert Group of Expert Consensus on Neoadjuvant Treatment of Breast Cancer in China (2021 edition). Expert consensus on neoadjuvant treatment of breast cancer in China (2021 edition)[J]. China Oncol, 2022, 32(1): 80-89. | |
| [2] |
BI Z, QIU P F, ZHANG Y, et al. A three lncRNA set: AC009975.1, POTEH-AS1 and AL390243.1 as nodal efficacy biomarker of neoadjuvant therapy for HER2 positive breast cancer[J]. Front Oncol, 2021, 11: 779140.
doi: 10.3389/fonc.2021.779140 |
| [3] |
樊庆达, 丛斌斌, 陈玉光, 等. 临床淋巴结阳性新辅助治疗后腋窝降阶处理的研究进展[J]. 中国癌症杂志, 2023, 33(2): 174-180.
doi: 10.19401/j.cnki.1007-3639.2023.02.011 |
| FAN Q D, CONG B B, CHEN Y G, et al. Research progress of axillary de-escalation management after neoadjuvant chemotherapy for clinical lymph node positive patients[J]. China Oncol, 2023, 33(2): 174-180. | |
| [4] |
BI Z, QIU P F, YANG T, et al. The modified shrinkage classification modes could help to guide breast conserving surgery after neoadjuvant therapy in breast cancer[J]. Front Oncol, 2022, 12: 982011.
doi: 10.3389/fonc.2022.982011 |
| [5] |
BURSTEIN H J, CURIGLIANO G, THÜRLIMANN B, et al. Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021[J]. Ann Oncol, 2021, 32(10): 1216-1235.
doi: 10.1016/j.annonc.2021.06.023 pmid: 34242744 |
| [6] |
GRADISHAR W J, MORAN M S, ABRAHAM J, et al. Breast cancer, version 3.2022, NCCN clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2022, 20(6): 691-722.
doi: 10.6004/jnccn.2022.0030 |
| [7] |
邱鹏飞, 王永胜. 前哨淋巴结时代乳腺癌的精准区域处理: 演进与展望[J]. 中国癌症杂志, 2022, 32(8): 680-687.
doi: 10.19401/j.cnki.1007-3639.2022.08.002 |
| QIU P F, WANG Y S. Precise regional management of breast cancer in the sentinel lymph node era: evolution and prospect[J]. China Oncol, 2022, 32(8): 680-687. | |
| [8] |
KUEMMEL S, HEIL J, RUELAND A, et al. A prospective, multicenter registry study to evaluate the clinical feasibility of targeted axillary dissection (TAD) in node-positive breast cancer patients[J]. Ann Surg, 2022, 276(5): e553-e562.
doi: 10.1097/SLA.0000000000004572 |
| [9] |
ARAGÓN-SÁNCHEZ S, CIRUELOS-GIL E, LÓPEZ-MARÍN L, et al. Feasibility of targeted axillary dissection for de-escalation of surgical treatment after neoadjuvant chemotherapy in breast cancer[J]. Surg Oncol, 2022, 44: 101823.
doi: 10.1016/j.suronc.2022.101823 |
| [10] |
BI Z, CHEN J J, LIU P C, et al. Candidates of genomic tests in HR + /HER2- breast cancer patients with 1-2 positive sentinel lymph node without axillary lymph node dissection: analysis from multicentric cohorts[J]. Front Oncol, 2021, 11: 722325.
doi: 10.3389/fonc.2021.722325 |
| [11] |
HARRISON B. Update on sentinel node pathology in breast cancer[J]. Semin Diagn Pathol, 2022, 39(5): 355-366.
doi: 10.1053/j.semdp.2022.06.016 pmid: 35803776 |
| [12] |
CHUNG H L, SUN J, LEUNG J W T. Breast cancer skip metastases: frequency, associated tumor characteristics, and role of staging nodal ultrasound in detection[J]. AJR Am J Roentgenol, 2021, 217(4): 835-844.
doi: 10.2214/AJR.20.24371 |
| [13] |
SUN J Y, YIN J, NING L S, et al. Clinicopathological characteristics of breast cancers with axillary skip metastases[J]. J Investig Surg, 2012, 25(1): 33-36.
doi: 10.3109/08941939.2011.598605 |
| [14] | 孙敬岩, 宁连胜. 乳腺癌腋窝淋巴结跳跃式转移的临床病理研究[J]. 中华肿瘤杂志, 2008, 30(5): 352-355. |
| SUN J Y, NING L S. Axillary skip metastases in breast cancer[J]. Chin J Oncol, 2008, 30(5): 352-355. | |
| [15] |
MOO T A, EDELWEISS M, HAJIYEVA S, et al. Is low-volume disease in the sentinel node after neoadjuvant chemotherapy an indication for axillary dissection?[J]. Ann Surg Oncol, 2018, 25(6): 1488-1494.
doi: 10.1245/s10434-018-6429-2 |
| [16] |
ALMAHARIQ M F, LEVITIN R, QUINN T J, et al. Omission of axillary lymph node dissection is associated with inferior survival in breast cancer patients with residual N1 nodal disease following neoadjuvant chemotherapy[J]. Ann Surg Oncol, 2021, 28(2): 930-940.
doi: 10.1245/s10434-020-08928-2 |
| [17] | 王永胜, 吴炅, 刘红, 等. 乳腺癌前哨淋巴结活检规范化操作指南(2022精要版)[J]. 中国肿瘤临床, 2022, 49(22): 1136-1142. |
| WANG Y S, WU J, LIU H, et al. Guidelines for standardized practice of sentinel lymph node biopsy in breast cancer (2022 abridged version)[J]. Chin J Clin Oncol, 2022, 49(22): 1136-1142. | |
| [18] |
COSTAZ H, BOULLE D, BERTAUT A, et al. Omitting axillary lymph node dissection after positive sentinel lymph node in the post-Z0011 era: compliance with NCCN and ASCO clinical guidelines and Z0011 criteria in a large prospective cohort[J]. Bull Cancer, 2022, 109(3): 268-279.
doi: 10.1016/j.bulcan.2021.09.018 |
| [19] |
KORDE L A, SOMERFIELD M R, CAREY L A, et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO guideline[J]. J Clin Oncol, 2021, 39(13): 1485-1505.
doi: 10.1200/JCO.20.03399 pmid: 33507815 |
| [20] |
VAN LOEVEZIJN A A, VAN DER NOORDAA M E M, STOKKEL M P M, et al. Three-year follow-up of de-escalated axillary treatment after neoadjuvant systemic therapy in clinically node-positive breast cancer: the MARI-protocol[J]. Breast Cancer Res Treat, 2022, 193(1): 37-48.
doi: 10.1007/s10549-022-06545-z |
| [21] | MONTAGNA G. OPBC-04/EUBREAST-06/OMA study[C]. SABCS, 2022, Abstract GS4-02. |
| [1] | WU Wen, ZHANG Ruoxin, WENG Junyong, MA Yanlei, CAI Guoxiang, LI Xinxiang, YANG Yongzhi. Exploring the prognostic value of positive lymph node ratio in stage Ⅲ colorectal cancer patients and establishing a predictive model [J]. China Oncology, 2024, 34(9): 873-880. |
| [2] | XU Rui, WANG Zehao, WU Jiong. Advances in the role of tumor-associated neutrophils in the development of breast cancer [J]. China Oncology, 2024, 34(9): 881-889. |
| [3] | CAO Xiaoshan, YANG Beibei, CONG Binbin, LIU Hong. The progress of treatment for brain metastases of triple-negative breast cancer [J]. China Oncology, 2024, 34(8): 777-784. |
| [4] | ZHANG Jian. Clinical consideration of two key questions in assessing menopausal status of female breast cancer patients [J]. China Oncology, 2024, 34(7): 619-627. |
| [5] | JIANG Dan, SONG Guoqing, WANG Xiaodan. Study on the mechanism of mitochondrial dysfunction and CPT1A/ERK signal transduction pathway regulating malignant behavior in breast cancer [J]. China Oncology, 2024, 34(7): 650-658. |
| [6] | DONG Jianqiao, LI Kunyan, LI Jing, WANG Bin, WANG Yanhong, JIA Hongyan. A study on mechanism of SIRT3 inducing endocrine drug resistance in breast cancer via deacetylating YME1L1 [J]. China Oncology, 2024, 34(6): 537-547. |
| [7] | HAO Xian, HUANG Jianjun, YANG Wenxiu, LIU Jinting, ZHANG Junhong, LUO Yubei, LI Qing, WANG Dahong, GAO Yuwei, TAN Fuyun, BO Li, ZHENG Yu, WANG Rong, FENG Jianglong, LI Jing, ZHAO Chunhua, DOU Xiaowei. Establishment of primary breast cancer cell line as new model for drug screening and basic research [J]. China Oncology, 2024, 34(6): 561-570. |
| [8] | XUE Chi, GAO Peng, ZHU Zhi, WANG Zhenning. Application and challenge of immunotherapy in perioperative therapy of gastric cancer [J]. China Oncology, 2024, 34(3): 259-267. |
| [9] | Committee of Breast Cancer Society, China Anti-Cancer Association. Expert consensus on clinical applications of ovarian function suppression for Chinese women with early breast cancer (2024 edition) [J]. China Oncology, 2024, 34(3): 316-333. |
| [10] | ZHANG Qi, XIU Bingqiu, WU Jiong. Progress of important clinical research of breast cancer in China in 2023 [J]. China Oncology, 2024, 34(2): 135-142. |
| [11] | ZHANG Siyuan, JIANG Zefei. Important research progress in clinical practice for advanced breast cancer in 2023 [J]. China Oncology, 2024, 34(2): 143-150. |
| [12] | WANG Zhaobu, LI Xing, YU Xinmiao, JIN Feng. Important research progress in clinical practice for early breast cancer in 2023 [J]. China Oncology, 2024, 34(2): 151-160. |
| [13] | LUO Yang, SUN Tao, SHAO Zhimin, CUI Jiuwei, PAN Yueyin, ZHANG Qingyuan, CHENG Ying, LI huiping, YANG Yan, YE Changsheng, YU Guohua, WANG Jingfen, LIU Yunjiang, LIU Xinlan, ZHOU Yuhong, BAI Yuju, GU Yuanting, WANG Xiaojia, XU Binghe, SONG Lihua. Efficacy, metabolic characteristics, safety and immunogenicity of AK-HER2 compared with reference trastuzumab in patients with metastatic HER2-positive breast cancer: a multicenter, randomized, double-blind phase Ⅲ equivalence trial [J]. China Oncology, 2024, 34(2): 161-175. |
| [14] | CHEN Yuanxiang, YU Tao, YANG Shiyu, ZENG Tao, WEI Lan, ZHANG Yan. KDM4A promotes the migration and invasion of breast cancer cell line MDA-MB-231 by downregulating BMP9 [J]. China Oncology, 2024, 34(2): 176-184. |
| [15] | HU Xiaoyu, CAI Yuwen, YE Fugui, SHAO Zhimin, HU Weigang, YU Keda. Impact of BRCA1/2 germline mutation on the incidence of second primary cancer following postoperative radiotherapy in patients with triple-negative breast cancer [J]. China Oncology, 2024, 34(2): 185-190. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd