Welcome to China Oncology,
China Oncology ›› 2022, Vol. 32 ›› Issue (2): 177-190.doi: 10.19401/j.cnki.1007-3639.2022.02.010
Chinese Anti-Cancer Association, Committee of Breast Cancer Society
Received:2021-11-15
Revised:2021-12-05
Online:2022-02-28
Published:2022-03-08
Share article
CLC Number:
Chinese Anti-Cancer Association, Committee of Breast Cancer Society. Expert consensus on clinical applications of ovarian function suppression for Chinese women with early breast cancer 2021 CACA-CBCS[J]. China Oncology, 2022, 32(2): 177-190.
"
| 《中国抗癌协会乳腺癌诊治指南与规范(2021版)》[ | 《中国绝经前女性乳腺癌患者辅助治疗后绝经判断标准及芳香化酶抑制剂临床应用共识(草案修正案)》[ |
|---|---|
| 年龄≥60岁患者 | 年龄≥50岁患者,化疗后或在服用SERM药物期间闭经至少12个月,且E2及 FSH水平连续测定至少3次均达到绝经后水平 |
| 年龄<60岁患者,自然停经≥12个月,在近1年未接受化 疗、他莫昔芬、托瑞米芬或卵巢去势的情况下,FSH和 E2水平在绝经后范围内 | 年龄在45~50岁患者,化疗后或在服用SERM药物期间闭经至少24个月,且 E2及FSH水平连续测定至少3次均达到绝经后水平 |
| 年龄<60岁正在服用他莫昔芬或托瑞米芬的患者,FSH和 E2水平在绝经后范围内 | 年龄小于45岁患者,由于卵巢功能恢复的概率较大,原则上不适用本标准 |
| 上述标准中年龄可参考患者家族女性平均停经年龄作出个例调整 |
"
"
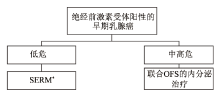
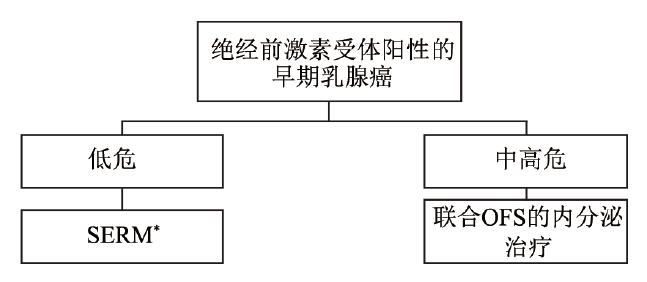
| 危险度 | 判别要点 | ||
|---|---|---|---|
| 转移淋巴结 | ER/PR | 其他情况 | |
| 低危 | 阴性 | 阳性 | 同时具备以下条件a:pT≤2 cm;组织学Ⅰ级;LVI阴性;HER2阴性;年龄≥35岁;Ki-67≤20%或实验室中位值; |
| HER2阴性且不满足上述条件,但多基因检测低危 | |||
| 中危 | 不符合低/高危定义的其他情况 | ||
| 高危 | 1~3枚阳性 | 阳性 | 具备以下条件之一b:组织学Ⅲ级;pT>5 cm;HER2阳性;多基因检测高危; |
| 阴性 | 任何情况 | ||
| ≥4枚阳性 | 任何情况 | 任何情况 | |
"
| 相关不良事件 | 药物治疗 | 非药物治疗 |
|---|---|---|
| 血管舒缩症状:潮热,盗汗 | SSRI帕罗西汀(不宜与SERM合用) SNRIs:文拉法辛 加巴喷丁 可乐定 中医中药 | 针灸 合适的衣物 |
| 阴道症状:阴道干燥,阴道萎缩 | 阴道雌激素△:Ovestin(阴道雌三醇) | 非激素润滑剂 阴道保湿霜 |
| 性功能障碍:性欲减退 | 非激素润滑剂,阴道保湿霜 | |
| 阴道雌激素:Ovestin(阴道雌三醇) | 充分的医患沟通 放松心情 | |
| 骨骼肌症状:骨质疏松,骨折 | 双膦酸盐,地舒单抗,维生素D和钙* | 负重练习 戒烟限酒 |
| 关节痛 | NSAID和COX-2抑制剂 维生素D | 减肥 全身抗阻力练习 物理治疗 |
| 精神系统症状:情绪变化,如抑郁 | SSRI(如西酞普兰,依他普仑) | |
| SNRIs(如文拉法辛) | 规律运动 均衡饮食 心理治疗 |
| [1] | 曹毛毛,, 陈万青. GLOBOCAN 2020全球癌症统计数据解读[J]. 中国医学前沿杂志(电子版), 2021,13(3):63-69. |
| CAO M M,, CHEN W Q. Interpretation on the global cancer statistics of GLOBOCAN 2020[J]. Chin J Front Med Sci Electron Version, 2021,13(3):63-69. | |
| [2] | FAN L,, STRASSER-WEIPPL K,, LI J J, et al. Breast cancer in China[J]. Lancet Oncol, 2014,15(7):e279-e289. |
| [3] | EARLY BREAST CANCER TRIALISTS’ COLLABORATIVE GROUP(EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials[J]. Lancet, 2005,365(9472):1687-1717. |
| [4] | DAVIES C,, PAN H C,, GODWIN J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial[J]. Lancet, 2013,381(9869):805-816. |
| [5] | GRAY R G,, REA D,, HANDLEY K, et al. aTTom: long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6, 953 women with early breast cancer[J]. J Clin Oncol, 2013,31(18_suppl):5. |
| [6] | LHRH-AGONISTS IN EARLY BREAST CANCER OVERVIEW GROUP, CUZICK J,, AMBROISINE L, et al. Use of luteinising-hormone-releasing hormone agonists as adjuvant treatment in premenopausal patients with hormone-receptor-positive breast cancer: a meta-analysis of individual patient data from randomised adjuvant trials[J]. Lancet, 2007,369(9574):1711-1723. |
| [7] | FRANCIS P A,, PAGANI O,, FLEMING G F, et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer[J]. N Engl J Med, 2018,379(2):122-137. |
| [8] | NOH W C,, LEE J W,, NAM S J, et al. Role of adding ovarian function suppression to tamoxifen in young women with hormone-sensitive breast cancer who remain premenopausal or resume menstruation after chemotherapy: the ASTRRA study[J]. J Clin Oncol, 2018,36(15_suppl):502. |
| [9] | PERRONE F,, DE LAURENTIIS M,, DE PLACIDO S, et al. The HOBOE-2 multicenter randomized phase Ⅲ trial in premenopausal patients with hormone-receptor positive early breast cancer comparing triptorelin plus either tamoxifen or letrozole or letrozole + zoledronic acid[J]. Ann Oncol, 2018, 29: viii704. |
| [10] | HARRISON G S,, WIERMAN M E,, NETT T M, et al. Gonadotropin-releasing hormone and its receptor in normal and malignant cells[J]. Endocr Relat Cancer, 2004,11(4):725-748. |
| [11] | DOISNEAU-SIXOU S F,, SERGIO C M,, CARROLL J S, et al. Estrogen and antiestrogen regulation of cell cycle progression in breast cancer cells[J]. Endocr Relat Cancer, 2003,10(2):179-186. |
| [12] | TAN S H,, WOLFF A C. Luteinizing hormone-releasing hormone agonists in premenopausal hormone receptor-positive breast cancer[J]. Clin Breast Cancer, 2007,7(6):455-464. |
| [13] | MCDONALD WADE S 3rd,, HACKNEY M H,, KHATCHERESSIAN J, et al. Ovarian suppression in the management of premenopausal breast cancer: methods and efficacy in adjuvant and metastatic settings[J]. Oncology, 2008,75(3/4):192-202. |
| [14] | 中国抗癌协会乳腺癌专业委员会. 中国抗癌协会乳腺癌诊治指南与规范(2021年版)[J]. 中国癌症杂志, 2021,31(10):954-1040. |
| The Society of Breast Cancer China Anti-cancer Association. Guidelines for breast cancer diagnosis and treatment by China Anti-cancer Association (2021 edition)[J]. China Oncol, 2021,31(10):954-1040. | |
| [15] | 中国抗癌协会乳腺癌专业委员会. 中国绝经前女性乳腺癌患者辅助治疗后绝经判断标准及芳香化酶抑制剂临床应用共识(草案修正案)[J]. 中国癌症杂志, 2011,21(5):418-420. |
| The Society of Breast Cancer China Anti-cancer Association. Postmenopausal criteria for menopausal women and clinical consensus on aromatase application in China’s pre-menopausal women with breast cancer (draft amendment)[J]. China Oncol, 2011,21(5):418-420. | |
| [16] | FRANCIS P A,, REGAN M M,, FLEMING G F, et al. Adjuvant ovarian suppression in premenopausal breast cancer[J]. N Engl J Med, 2015,372(5):436-446. |
| [17] | DEES E C,, DAVIDSON N E. Ovarian ablation as adjuvant therapy for breast cancer[J]. Semin Oncol, 2001,28(4):322-331. |
| [18] | JONAT W,, KAUFMANN M,, SAUERBREI W, et al. Goserelin versus cyclophosphamide, methotrexate, and fluorouracil as adjuvant therapy in premenopausal patients with node-positive breast cancer: the Zoladex Early Breast Cancer Research Association Study[J]. J Clin Oncol, 2002,20(24):4628-4635. |
| [19] | BUI K T,, WILLSON M L,, GOEL S, et al. Ovarian suppression for adjuvant treatment of hormone receptor-positive early breast cancer[J]. Cochrane Database Syst Rev, 2020, 3: CD013538. |
| [20] | BURSTEIN H J,, LACCHETTI C,, ANDERSON H, et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American Society of Clinical Oncology clinical practice guideline update on ovarian suppression[J]. J Clin Oncol, 2016,34(14):1689-1701. |
| [21] | THOMSSEN C,, BALIC M,, HARBECK N, et al. St. Gallen/Vienna 2021: a brief summary of the consensus discussion on customizing therapies for women with early breast cancer[J]. Breast Care (Basel), 2021,16(2):135-143. |
| [22] | PALUCH-SHIMON S,, CARDOSO F,, PARTRIDGE A H, et al. ESO-ESMO 4th International Consensus Guidelines for Breast Cancer in Young Women (BCY4)[J]. Ann Oncol, 31(6):674-696. |
| [23] | CARDOSO F,, KYRIAKIDES S,, OHNO S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2019,30(8):1194-1220. |
| [24] | Lan B,, Ma F, et al. Int J Cancer, 2018, 143:184;J Clin Oncol, 2007, 1;25(25):3837-3845; Ann Oncol, 2008,19(8):1423-1429. |
| [25] | EARLY BREAST CANCER TRIALISTS’ COLLABORATIVE GROUP(EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials[J]. Lancet, 2015,386(10001):1341-1352. |
| [26] | REGAN M M,, FRANCIS P A,, PAGANI O, et al. Absolute benefit of adjuvant endocrine therapies for premenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative early breast cancer: TEXT and SOFT trials[J]. J Clin Oncol, 2016,34(19):2221-2231. |
| [27] | REGAN M M,, FRANCIS P A,, PAGANI O, et al. Absolute improvements in freedom from distant recurrence with adjuvant endocrine therapy for premenopausal women with HR + HER2 -negative breast cancer: results from TEXT and SOFT [J]. J Clin Oncol, 2018,36(suppl 15):503-503. |
| [28] | LAMBERTINI M,, BONI, MICHELOTTI A, et al. Ovarian suppression with triptorelin during adjuvant breast cancer chemotherapy and long-term ovarian function, pregnancies, and disease-free survival: a randomized clinical trial[J]. JAMA, 2015,314(24):2632-2640. |
| [29] | LAMBERTINI M,, MOORE H C F,, LEONARD R C F, et al. Gonadotropin-releasing hormone agonists during chemotherapy for preservation of ovarian function and fertility in premenopausal patients with early breast cancer: a systematic review and meta-analysis of individual patient-level data[J]. J Clin Oncol, 2018,36(19):1981-1990. |
| [30] | PAN H C,, GRAY R,, BRAYBROOKE J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years[J]. N Engl J Med, 2017,377(19):1836-1846. |
| [31] | NCCN Clinical Practice Guidelines in Oncology(NCCN Guidelines®). Breast Cancer, Version 1. 2022[EB/OL]. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419[2021]. |
| [32] | HICKEY M,, SAUNDERS C,, PARTRIDGE A, et al. Practical clinical guidelines for assessing and managing menopausal symptoms after breast cancer[J]. Ann Oncol, 2008,19(10):1669-1680. |
| [33] | LOIBL S,, LINTERMANS A,, DIEUDONNÉ A S, et al. Management of menopausal symptoms in breast cancer patients[J]. Maturitas, 2011,68(2):148-154. |
| [34] | PETREK J A,, NAUGHTON M J,, CASE L D, et al. Incidence, time course, and determinants of menstrual bleeding after breast cancer treatment: a prospective study[J]. J Clin Oncol, 2006,24(7):1045-1051. |
| [35] | LIEM G S,, MO F K,, PANG E, et al. Chemotherapy-related amenorrhea and menopause in young Chinese breast cancer patients: analysis on incidence, risk factors and serum hormone profiles[J]. PLoS One, 2015,10(10):e0140842. |
| [36] | SMITH I E,, DOWSETT M,, YAP Y S, et al. Adjuvant aromatase inhibitors for early breast cancer after chemotherapy-induced amenorrhoea: caution and suggested guidelines[J]. J Clin Oncol, 2006,24(16):2444-2447. |
| [37] | 宋三泰,, 陈建魁,, 单彬. 规范乳腺癌性激素化验报告理顺应用AIs的绝经标准[J]. 中华乳腺病杂志(电子版), 2012,6(3):238-243. |
| SONG S T,, CHEN J K,, SHAN B. To standardize the sex hormone test report of breast cancer and straighten out the application of AIs’s menopausal standard[J]. Chin J Breast Dis Electron Ed, 2012,6(3):238-243. | |
| [38] | 江泽飞,, 王晓迪. 乳腺癌内分泌治疗十个热点问题的思考[J]. 中华外科杂志, 2015,2(12):895-900. |
| JIANG Z F,, WANG X D. Consideration and discussion on ten hot issues of endocrine therapy for breast cancer[J]. Chin J Surg, 2015,2(12):895-900. | |
| [39] | GNANT M,, MLINERITSCH B,, STOEGER H, et al. Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 62-month follow-up from the ABCSG-12 randomised trial[J]. Lancet Oncol, 2011,12(7):631-641. |
| [40] | MOORE H C,, UNGER J M,, PHILLIPS K A, et al. Goserelin for ovarian protection during breast-cancer adjuvant chemotherapy[J]. N Engl J Med, 2015,372(10):923-932. |
| [41] | MOORE H C F,, UNGER J M,, PHILLIPS K A, et al. Final analysis of the prevention of early menopause study (POEMS)/SWOG intergroup S0230[J]. J Natl Cancer Inst, 2019,111(2):210-213. |
| [42] | DEL MASTRO L,, BONI, MICHELOTTI A, et al. Effect of the gonadotropin-releasing hormone analogue triptorelin on the occurrence of chemotherapy-induced early menopause in premenopausal women with breast cancer: a randomized trial[J]. JAMA, 2011,306(3):269-276. |
| [43] | LAMBERTINI M,, BONI L C,, MICHELOTTI A, et al. Ovarian suppression with triptorelin during adjuvant breast cancer chemotherapy and long-term ovarian function, pregnancies, and disease-free survival[J]. JAMA, 2015,314(24):2632. |
| [44] | LAMBERTINI M,, BONI L,, MICHELOTTI A, et al. Final analysis of the PROMISE-GIM6 phase Ⅲ trial assessing GnRH agonist use during chemotherapy as a strategy to preserve ovarian function in premenopausal patients with early breast cancer[J]. J Clin Oncol, 39(suppl 15):516-516. |
| [45] | LAMBERTINI M,, MOORE H C F,, LEONARD R C F, et al. Gonadotropin-releasing hormone agonists during chemotherapy for preservation of ovarian function and fertility in premenopausal patients with early breast cancer: a systematic review and meta-analysis of individual patient-level data[J]. J Clin Oncol, 2018,36(19):1981-1990. |
| [46] | PALUCH-SHIMON S,, CARDOSO F,, PARTRIDGE A H, et al. ESO-ESMO 4th international consensus guidelines for breast cancer in young women (BCY4)[J]. Ann Oncol, 2020,31(6):674-696. |
| [47] | CARDOSO F,, KYRIAKIDES S,, OHNO S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2019,30(10):1674. |
| [48] | 中国年轻乳腺癌诊疗与生育管理专家共识专家委员会. 年轻乳腺癌诊疗与生育管理专家共识[J]. 中华肿瘤杂志, 2019,41(7):486-495. |
| Expert Committee on China’s Young Breast Cancer Diagnosis and Treatment and Fertility Management Expert Consensus. Expert consensus on diagnosis and treatment and birth management for young breast cancer[J]. Chin J Oncol, 2019,41(7):486-495. | |
| [49] | Premenopausal women with breast cancer: developing drugs for treatment guidance for industry[P]. FDA, 2020, 2020-D-1553. |
| [50] | GAO J J,, KROL D,, NARAYAN P, et al. Bringing safe and effective therapies to premenopausal women with breast cancer: efforts to broaden eligibility criteria[J]. Ann Oncol, 2021,32(8):950-953. |
| [1] | XU Rui, WANG Zehao, WU Jiong. Advances in the role of tumor-associated neutrophils in the development of breast cancer [J]. China Oncology, 2024, 34(9): 881-889. |
| [2] | Committee of Integrated Rehabilitation for Urogenital Tumors, Chinese Anti-Cancer Association. Chinese expert consensus on perioperative integrated rehabilitation for radical prostatectomy (2024 edition) [J]. China Oncology, 2024, 34(9): 890-902. |
| [3] | CAO Xiaoshan, YANG Beibei, CONG Binbin, LIU Hong. The progress of treatment for brain metastases of triple-negative breast cancer [J]. China Oncology, 2024, 34(8): 777-784. |
| [4] | ZHANG Jian. Clinical consideration of two key questions in assessing menopausal status of female breast cancer patients [J]. China Oncology, 2024, 34(7): 619-627. |
| [5] | JIANG Dan, SONG Guoqing, WANG Xiaodan. Study on the mechanism of mitochondrial dysfunction and CPT1A/ERK signal transduction pathway regulating malignant behavior in breast cancer [J]. China Oncology, 2024, 34(7): 650-658. |
| [6] | Cancer Nuclear Medicine Committee of China Anti-Cancer Association, Chinese Association of Nuclear Medicine Physicians. Expert consensus of 177Lu-labeled PSMA radioligand therapy for clinical practice of prostate cancer (2024 edition) [J]. China Oncology, 2024, 34(7): 702-714. |
| [7] | DONG Jianqiao, LI Kunyan, LI Jing, WANG Bin, WANG Yanhong, JIA Hongyan. A study on mechanism of SIRT3 inducing endocrine drug resistance in breast cancer via deacetylating YME1L1 [J]. China Oncology, 2024, 34(6): 537-547. |
| [8] | HAO Xian, HUANG Jianjun, YANG Wenxiu, LIU Jinting, ZHANG Junhong, LUO Yubei, LI Qing, WANG Dahong, GAO Yuwei, TAN Fuyun, BO Li, ZHENG Yu, WANG Rong, FENG Jianglong, LI Jing, ZHAO Chunhua, DOU Xiaowei. Establishment of primary breast cancer cell line as new model for drug screening and basic research [J]. China Oncology, 2024, 34(6): 561-570. |
| [9] | Professional Committee on Gastric Cancer of Shanghai Anticancer Association , Professional Committee on Gastrointestinal Cancer of China Association for Promotion of Health Science and Technology . Chinese expert consensus on clinical practice of locally advanced gastric cancer invading adjacent organs (2024 edition) [J]. China Oncology, 2024, 34(5): 517-526. |
| [10] | Committee of Breast Cancer Society, China Anti-Cancer Association. Expert consensus on clinical applications of ovarian function suppression for Chinese women with early breast cancer (2024 edition) [J]. China Oncology, 2024, 34(3): 316-333. |
| [11] | ZHANG Qi, XIU Bingqiu, WU Jiong. Progress of important clinical research of breast cancer in China in 2023 [J]. China Oncology, 2024, 34(2): 135-142. |
| [12] | ZHANG Siyuan, JIANG Zefei. Important research progress in clinical practice for advanced breast cancer in 2023 [J]. China Oncology, 2024, 34(2): 143-150. |
| [13] | WANG Zhaobu, LI Xing, YU Xinmiao, JIN Feng. Important research progress in clinical practice for early breast cancer in 2023 [J]. China Oncology, 2024, 34(2): 151-160. |
| [14] | LUO Yang, SUN Tao, SHAO Zhimin, CUI Jiuwei, PAN Yueyin, ZHANG Qingyuan, CHENG Ying, LI huiping, YANG Yan, YE Changsheng, YU Guohua, WANG Jingfen, LIU Yunjiang, LIU Xinlan, ZHOU Yuhong, BAI Yuju, GU Yuanting, WANG Xiaojia, XU Binghe, SONG Lihua. Efficacy, metabolic characteristics, safety and immunogenicity of AK-HER2 compared with reference trastuzumab in patients with metastatic HER2-positive breast cancer: a multicenter, randomized, double-blind phase Ⅲ equivalence trial [J]. China Oncology, 2024, 34(2): 161-175. |
| [15] | CHEN Yuanxiang, YU Tao, YANG Shiyu, ZENG Tao, WEI Lan, ZHANG Yan. KDM4A promotes the migration and invasion of breast cancer cell line MDA-MB-231 by downregulating BMP9 [J]. China Oncology, 2024, 34(2): 176-184. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd