Welcome to China Oncology,
China Oncology ›› 2023, Vol. 33 ›› Issue (5): 527-548.doi: 10.19401/j.cnki.1007-3639.2023.05.013
• Guideline and Concensus • Previous Articles
Expert Committee on Immunotherapy of Chinese Society of Clinical Oncology , Professional Committee on Cancer Biotherapy of Shanghai Anticancer Association
Received:2023-01-12
Revised:2023-02-25
Online:2023-05-30
Published:2023-06-16
Share article
CLC Number:
Expert Committee on Immunotherapy of Chinese Society of Clinical Oncology , Professional Committee on Cancer Biotherapy of Shanghai Anticancer Association . Chinese expert consensus on clinical application of recombinant oncolytic adenovirus in the treatment of malignant tumors[J]. China Oncology, 2023, 33(5): 527-548.
"
| 证据级别 | 研究设计类型 | 描述 |
|---|---|---|
| 1级 | RCT/实验性研究 | 1a:多项RCT的SR; 1b:多项RCT及其他干预性研究的SR; 1c:单项RCT; 1d:准RCT |
| 2级 | 类实验性研究 | 2a:多项类实验性研究的SR; 2b:多项类实验性研究及其他低质量干预性研究的SR; 2c:单项前瞻性有对照组的类实验性研究; 2d:前后对照/回顾性对照的类实验性研究 |
| 3级 | 观察性-分析性研究 | 3a:多项队列研究的SR; 3b:多项队列研究及其他低质量观察性研究的SR; 3c:单项有对照组的队列研究; 3d:单项病例对照研究; 3e:单项无对照组的观察性研究 |
| 4级 | 观察性-描述性研究 | 4a:多项描述性研究的SR; 4b:单项横断面研究; 4c:病例系列研究; 4d:个案研究 |
| 5级 | 专家意见/基础研究 | 5a:对专家意见的SR; 5b:专家共识; 5c:基础研究/单项专家意见 |
"
| 问卷批次 | 一 | 二 | 三 | 四 | 汇总去重 |
|---|---|---|---|---|---|
| 陈述(条) | 27 | 25 | 44 | 45 | 47 |
| 参与专家(人) | 11 | 16 | 30 | 40 | 86 |
| 修改建议(条) | 38 | 28 | 45 | 28 | 123 |
"
| 产品名称 | 研发公司/机构 | 临床阶段 | 给药方式 | 主要适应证 |
|---|---|---|---|---|
| H101 | 上海三维生物技术有限公司 | 已上市 | 瘤内注射 | 鼻咽癌 |
| H103 | 上海三维生物技术有限公司 | Ⅰ | 瘤内注射 | 晚期实体瘤 |
| KH901 | 成都康弘生物科技有限公司 | Ⅱ | 瘤内注射 | 头颈癌 |
| ADV-TK | 深圳市天达康基因工程有限公司, 武汉天达康生物技术有限公司 | Ⅲ | 静脉注射 | 肝部肿瘤 |
| EDS01 | 成都恩多施生物工程技术有限公司, 贵州百灵企业集团制药股份有限公司 | Ⅱ | 瘤内注射 | 鼻咽肿瘤 |
| E10A | 广州达博生物制品有限公司 | Ⅲ | 瘤内注射 | 头颈部鳞癌 |
| OBP301 | 江苏恒瑞医药股份有限公司 | Ⅰ、Ⅱ | 瘤内注射 | 黑色素瘤 |
"
| 研究类型 | 纳入患者 | 干预措施 | 主要结果 | 证据级别 |
|---|---|---|---|---|
| Ⅲ期RCT[ | 160例头颈、食管鳞癌患者a | H101联合化疗b vs 单纯化疗b | H101联合一线化疗方案的总有效率显著高于单纯化疗组(78.8% vs 39.6%,P=0.000),两组相差达39.2%,此差异相比于包括一线及二线化疗的联合组与单药化疗组之间总有效率的差异更加明显(72.7% vs 40.4%),提示H101对一线病例的疗效较好;但联合组鼻咽癌患者的有效率与单纯化疗组相比差异无统计学意义,可能与纳入的鼻咽癌患者总例数较少有关。 | 1c |
| 观察性研究[ | 54例鼻咽癌患者c | H101联合化疗b | 联合治疗的总有效率为77.7%,其中初治组的总有效率为81.3%,复治组为50.0%,提示H101对初治患者的疗效较好,但由于复治组病例较少,未能进行统计学分析;不同疾病分期之间,Ⅱ、Ⅲ和Ⅳ期的有效率分别为87.5%、68.7%和50.0%,提示就诊时分期越早疗效越好 | 2c |
"
| 研究类型 | 纳入患者 | 干预措施 | 主要结果 | 证据级别 |
|---|---|---|---|---|
| 回顾性研究[ | 187例HCC患者a | TACE联合H101 vs TACE | TACE联合H101治疗相比单用TACE治疗的CR率(28.7% vs 14.8%)和PR率(32.2% vs 21.6%)更高、SD率(26.4% vs 38.6%)和PD率(12.6% vs 25%)更低,此外,联合组的中位OS(12.8个月 vs 11.6个月,P=0.046)和PFS(10.49个月 vs 9.72个月,P=0.044)均显著长于单用TACE组 | 3c |
| 回顾性研究[ | 476例HCC患者a | TACE联合H101 vs TACE | TACE联合H101治疗相比单用TACE治疗可延长HCC患者的中位OS(1、2、3年的生存率分别为61.0% vs 55.0%、40.0% vs 33.4%、31.5% vs 22.3%),并降低癌症特异性死亡率(1、2、3年的癌症特异性死亡率分别为37.3% vs 42.0%、55.7% vs 63.5%、61.9% vs 74.7%),多变量竞争风险分析确定TACE联合H101治疗是降低癌症特异性死亡率的独立因素 | 3c |
"
| 研究类型 | 纳入患者 | 干预措施 | 主要结果 | 证据级别 |
|---|---|---|---|---|
| Meta分析a[ | 2 289例黑色素瘤患者 | T-VEC vs 伊匹单抗 vs 维莫非尼 | T-VEC治疗转移性黑色素瘤的中位OS与伊匹单抗和维莫非尼类似甚至更好,且在无骨、脑、肺或其他内脏转移的患者中改善更明显 | 1a |
| Ⅲ期RCT[ | 436例黑色素瘤患者b | T-VEC vs GM-CSF | 病灶内注射T-VEC组患者的DRR(16.3% vs 2.1%,P<0.001)、总缓解率(26.4% vs 5.7%,P<0.001)和中位OS(23.3个月 vs 18.9个月,P=0.051)均高于GM-CSF对照组;亚组分析数据显示,T-VEC的疗效(DRR和中位OS)在ⅢB、ⅢC、ⅣM1a期患者和既往未接受过治疗的患者中更显著 | 1c |
| Ⅱ期RCT[ | 198例黑色素瘤患者 | T-VEC联合伊匹单抗 | T-VEC和伊匹单抗联合治疗组的ORR显著高于伊匹单抗单药治疗组(39% vs 18%,P=0.002),亚组分析的结果显示,在BRAF野生型患者中,联合组的ORR显著高于伊匹单抗治疗组(42% vs 10%,P<0.001),但在BRAF突变型中,两组的ORR差异无统计学意义(34% vs 32%,P=1.000);提示T-VEC在BRAF野生型患者中的疗效更好;此外,联合治疗组的注射和未注射病变(包括内脏病变)均出现应答,联合组脏器病变减少的患者比例为52%,高于单药组的23% | 1c |
"
| 研究类型 | 纳入患者 | 干预措施 | 主要结果 | 证据级别 |
|---|---|---|---|---|
| Meta分析a[ | 1 494例肿瘤患者 | 溶瘤病毒联合传统一线治疗 vs 单用传统治疗 | 溶瘤病毒联合传统一线治疗相比单用传统治疗可显著提高ORR,虽然联合治疗增加了部分不良反应,但与联合治疗带来的益处相比,不良反应可以耐受 | 1a |
| Meta分析b[ | 1 939例肿瘤患者 | 溶瘤病毒联合化疗或靶向治疗或ICI vs 单用化疗或靶向治疗或ICI | 与单独化疗或使用靶向药物治疗相比,溶瘤病毒联合化疗或靶向药物未改善疗效;但溶瘤病毒与ICI(非化疗或靶向治疗)联合给药倾向于提供更好的ORR,而不会引起重度不良反应 | 1a |
| Ⅱ期RCT[ | 80例转移性乳腺癌患者 | Pelareorep联合紫杉醇 vs 紫杉醇 | Pelareorep与紫杉醇联合使用未改善PFS(主要终点),但可显著延长中位OS | 1c |
| Ⅱ期RCT[ | 198例黑色素瘤患者 | T-VEC联合伊匹单抗 vs 伊匹单抗 | T-VEC与伊匹单抗联合相比伊匹单抗单药治疗可显著提高黑色素瘤患者的ORR,且联合组中脏器病变减少的患者比例更高 | 1c |
| Ⅲ期RCT[ | 692例黑色素瘤患者 | T-VEC联合帕博利珠单抗 vs 安慰剂联合帕博利珠单抗 | 研究未达到主要终点,与安慰剂和帕博利珠单抗相比,T-VEC联合帕博利珠单抗并没有显著改善中位PFS和OS,两组之间的中位PFS相差5.8个月 | 1c |
| Ⅰb期临床试验[ | 21例黑色素瘤患者 | T-VEC联合帕博利珠单抗 | 患者耐受性良好,未出现剂量限制性毒性,ORR为62%,CR率为33%,研究还发现,溶瘤病毒可通过改变肿瘤微环境(CD8+ T淋巴细胞增加,PD-L1蛋白和IFN-γ表达量升高)来提高PD-1抗体的疗效 | 2d |
| Ⅰb期临床试验[ | 15例Ⅳ期黑色素瘤肝转移患者 | OrienX010联合特瑞普利单抗 | OrienX010联合特瑞普利单抗在黑色素瘤肝转移中表现出显著的病理学反应和良好的耐受性 | 2d |
| Ⅰb期临床试验[ | 30例可切除的ⅢB~ⅣM1a期肢端黑色素瘤患者 | OrienX010联合特瑞普利单抗 | OrienX010联合特普瑞利单抗作为新辅助治疗耐受性良好,病理学反应率较高,无患者复发,研究仍在继续评估无复发生存率 | 2d |
| 单臂单中心前瞻性研究[ | 10例黑色素瘤患者 | H101联合特瑞普利单抗 | H101联合特瑞普利单抗对晚期和难治性黑色素瘤患者具有可接受的不良反应和良好的抗肿瘤疗效,并促进血清IL-6、IL-8、IL-10和TNF-α发生有利变化 | 2d |
| 病例报道[ | 1例非小细胞肺癌患者 | H101联合纳武利尤单抗 | 1例对ICI(纳武利尤单抗)耐药的复发性非小细胞肺癌患者,在尝试免疫治疗加化疗或抗血管生成治疗后,出现一过性反应,PD后接受H101联合纳武利尤单抗治疗,疾病得到控制 | 4d |
"
| 瘤种 | 研究类型 | 病毒类型 | 主要结果 | 证据级别 |
|---|---|---|---|---|
| 肝转移癌 | Ⅰ期临床试验[ | 腺病毒H101 | 肝转移瘤内注射H101联合标准治疗(贝伐珠单抗联合mFOLFOX6/FOLFIRI)应用于不可切除的结直肠腺癌肝转移患者总体安全性良好,未发生4级以上不良反应,未观察到剂量相关毒性;联合H101治疗后各剂量组的肿瘤指标CEA均有所下降,中剂量组有1例影像学评价达到PR,未观察到明显的量效关系。目前正在开展Ⅱ期试验(ChiCTR1900027922),以进一步评价H101在结直肠癌肝转移患者中的疗效 | 2c |
| Ⅰ/Ⅱ期临床试验[ | 单纯疱疹病毒NV1020 | 肝动脉注射NV1020可稳定转移性结直肠癌患者的肝转移,且毒性极小,并可能使转移灶对挽救性化疗重新敏感 | 2d | |
| 基础研究[ | 腺病毒AV22EL | AV22EL可特异性地诱导表达A33的人结直肠癌细胞系的体外裂解,AV22EL在>90%的结直肠癌小鼠中完全消除了已建立的肝转移灶,肝功能生化指标恢复正常;其全身给药仅在肝转移中诱导E1A表达,而在正常器官中未诱导E1A表达 | 5c | |
| 胶质瘤 | Ⅰ期临床试 验[ | 腺病毒ONYX-015 | 将ONYX-015注射到复发恶性胶质瘤患者的瘤周区域,患者耐受性良好,纳入的24例患者均未发生与ONYX-015治疗相关的严重不良反应,在1010 pfu下未达到最大耐受剂量;随访19个月以上,1/6例ONYX-015注射剂量为109 pfu的受试者和2/6例注射剂量为1010 pfu的受试者仍存活,在ONYX-015注射后3个月接受第2次切除的2例患者中,观察到淋巴细胞和浆细胞样细胞浸润 | 2d |
| Ⅰ期临床试 验[ | 腺病毒H101 | 纳入的21例脑胶质瘤患者对术后瘤腔内注射H101的耐受性良好,未见严重不良反应,主要不良反应为发热,且血常规、血液生化、尿常规检查均未发现相关异常,表明瘤内注射H101在脑胶质瘤患者中有良好的安全性 | 2d | |
| Ⅰ期临床试验[ | 腺病毒DNX-2401 | 纳入的37例复发恶性胶质瘤患者中,有72%的患者(18/25)肿瘤减少;中位OS为9.5个月,有5例患者(20%)存活3年以上,其中3例患者CR,2例患者SD | 2d | |
| 恶性胸腹腔积液 | RCT[ | 腺病毒H101 | 与顺铂相比,H101治疗肺癌恶性胸腔积液患者的有效率更高(69.23% vs 53.84%,P<0.05),不良反应明显较轻 | 1c |
| RCT[ | 腺病毒H101 | 与中药组a、顺铂组和H101组相比,H101联合中药治疗组对肺癌伴恶性胸水的疗效最佳 | 1c | |
| 回顾性观察性研究[ | 腺病毒H101 | 40例恶性腹水患者接受H101腹腔注射后,腹水缓解率和控制率分别为40%和75%,其中5例(12.5%)患者腹水完全消失;主要不良反应为轻度至中度腹痛(8/40,20.0%)和发热(11/40,27.5%),未见3/4级不良反应;腹腔注射H101使腹水肿瘤细胞显著减少,树突状细胞和CD8+ T淋巴细胞数增加 | 3e | |
| 病例系列研究[ | 腺病毒H101 | 腹腔内注射H101耐受性良好,未见严重不良反应,与治疗前相比,H101治疗后显著增加了穿刺间隔时间(39.9±11.6)d vs (12.0±3.4)d,P <0.001],9例患者中有3例CR,2例PR,在单药H101治疗的4例患者中有1例CR,1例PR,H101联合顺铂治疗的5例患者中有2例CR,1例PR,提示H101联合化疗治疗恶性腹水的疗效可能更佳 | 4c | |
| 基础研究[ | VSV | VSV给药显著抑制了腹水形成,并延长了小鼠的生存期;VSV在腹水癌细胞中的复制明显增强,这可能是由于腹膜癌的代谢适应过程,如高糖酵解活性和谷氨酰胺代谢,有利于VSV复制 | 5c | |
| 胰腺癌 | Ⅰ/Ⅱ期临床试验[ | 腺病毒ONYX-015 | ONYX-015单用或与吉西他滨联合治疗不可切除胰腺癌患者的耐受性良好,联合治疗后,21例患者中有2例患者的注射肿瘤出现部分消退,2例轻度缓解,6例SD,11例PD或因治疗毒性而退出研究 | 2d |
| 类实验性研 究[ | 腺病毒H101 | H101联合吉西他滨组治疗4、12个月后的有效率均显著高于吉西他滨单药化疗组(4个月:40.0% vs 16.7%;12个月:62.5% vs 20.0%;P <0.05),联合治疗组12个月内病死率显著低于单药化疗组(60.0% vs 80.8%,P=0.028),中位生存期较单药化疗组显著延长[(8.8±0.5)个月 vs (7.6±0.4)个月,P=0.046],提示超声内镜引导下瘤体内注射H101联合吉西他滨治疗中晚期胰腺癌安全且有效 | 2d | |
| Ⅰb期临床试验[ | 呼肠病毒pelareorep | 11例一线治疗后进展的胰腺导管腺癌患者,静脉注射pelareorep联合帕博利珠单抗与化疗,在10例可评价疗效的患者中有3例达到疾病控制,其中1例PR(17.4个月),2例SD,分别持续9和4个月,治疗耐受性良好,大多为1或2级治疗相关不良反应。进一步评估pelareorep及抗PD-1抗体疗效的研究正在开展中 | 2c | |
| Ⅰb期临床试验[ | Ⅰ型单纯疱疹病毒HF10 | HF10联合厄洛替尼与吉西他滨治疗不可切除的局部晚期胰腺癌患者,在完成治疗的9例受试者中,3例部分应答,4例SD,2例PD,中位PFS为6.3个月,中位OS为15.5个月 | 2c | |
| MPM | Ⅰ/Ⅱa期临床试验[ | 疱疹病毒HSV1716 | 胸膜内导管注射HSV1716的耐受性良好,并出现抗肿瘤免疫反应,8周时50%的患者SD | 2d |
| 基础研究[ | 麻疹病毒 | 发挥关键抗病毒作用的IFN-Ⅰ(主要是IFN-a和IFN-b)基因纯合子缺失是MPM的频发事件,且与溶瘤性麻疹病毒治疗的高敏感性相关,更重要的是,研究发现IFN-Ⅰ基因纯合子缺失与肿瘤抑制基因CDKN2A的纯合子缺失共同发生,突出了在携带CDKN2A纯合缺失的MPM中进行溶瘤治疗的前景,但需注意的是,CDKN2A与IFN-Ⅰ基因纯合子缺失并不是调控溶瘤病毒敏感性的唯一机制 | 5c | |
| 子宫颈癌 | 回顾性观察性研究[ | 腺病毒H101(单用或联合放疗和其他药物治疗) | 22例子宫颈癌、2例阴道癌、2例外阴癌和2例卵巢癌病灶内注射H101后均有应答;治疗后3个月时局部病灶清除率为44.8%,ORR为72.4%;6个月时DRR和PFS率分别为88.1%和74.6%,12个月时DRR和PFS率分别为70.5%和62.2%;治疗相关不良反应多为1或2级(90.5%),最常见的不良反应为发热(70%)。临床严重不良反应少见(3级为7.9%,4级为1.6%);未见治疗相关死亡事件 | 3e |
| 病例报道[ | 腺病毒H101 | 1例患者在外照射放疗联合化疗(顺铂)后子宫颈肿瘤体积减小不明显,在局部瘤内注射H101后子宫颈肿瘤体积显著减小,之后接受2个周期局部瘤内注射H101联合近距离放疗和化疗(顺铂和紫杉醇),7个月随访时达到CR;未见严重不良反应 | 4d | |
| 基础研究[ | 腺病毒Ad-KFH | Ad-KFH能在产生SCCA2的子宫颈癌细胞中特异性复制并裂解癌细胞。此外,在子宫颈癌腹膜转移肿瘤模型中,Ad-KFH能延缓NOD-scid小鼠肿瘤生长,延长荷瘤小鼠的生存期,尤其是与顺铂联合时 | 5c | |
| 基础研究[ | 腺病毒H101 | H101能有效提高放疗对子宫颈癌细胞的抗肿瘤作用,可作为一种新型的子宫颈癌联合治疗药物 | 5c | |
| 基础研究[ | 单纯疱疹病毒T-01 | T-01对人子宫颈癌细胞株具有较高的细胞毒性,显著抑制子宫颈癌模型小鼠肿瘤的生长 | 5c | |
| 膀胱癌 | Ⅱ期临床试 验[ | 腺病毒CG0070 | 45例NMIBC患者治疗6个月后CR率为47%(32%~62%),其中CIS患者的CR率为58%(37%~78%),CIS±Ta/T1期患者为50%(33%~67%),单纯Ta/T1期患者为33%(8%~70%),此外1例Ta/T1期患者发展为肌层浸润性膀胱癌,单纯T1期患者未达到6个月CR率,提示NMIBC患者尤其是单纯CIS患者可能对CG0070有明显应答;治疗相关不良反应主要包括膀胱痉挛(36.0%)、血尿(28.0%)、排尿困难(25.0%)和尿急(22.0%),类免疫相关不良反应包括流感样症状(12.0%)和疲乏(6.0%),其中3级治疗相关不良反应包括排尿困难(3.0%)和低血压(1.5%),无4/5级治疗相关不良反应,提示卡介苗治疗无反应的高风险NMIBC患者能耐受CG0070毒性 | 2c |
| Ⅰ期临床试 验[ | 腺病毒CG0070 | 35例NMIBC患者在单次或多次膀胱内注射不同剂量CG0070后,尿液中检测到CG0070基因组增加和GM-CSF,CR率和中位CR时间分别为48.6%(17/35)和10.4个月;其中单次膀胱内注射组58.3%的患者在第2~5天时尿液CG0070基因组增加(7/12)(提示病毒复制);多次膀胱注射组的CR率为63.6%(14/22),临界或高磷酸化视网膜母细胞瘤的患者CR率达81.8%(9/11);所有患者最常见不良反应为1/2级膀胱毒性 | 2c |
"
| 研究类型 | 病毒名称 | 主要结果 | 证据级别 |
|---|---|---|---|
| 基础研究[ | ONYX-015 | ONYX-015在体外p53野生型和突变型细胞中均可复制,但该病毒在体内对突变型p53肿瘤表现出更强的抗肿瘤活性 | 5c |
| Ⅱ期临床试验[ | ONYX-015 | p53突变型肿瘤(7/12)比p53野生型肿瘤(0/7)更可能发生ONYX-015诱导的坏死(P=0.017) | 2d |
| 基础研究[ | ONYX-015 | ONYX-015在肿瘤细胞中的选择性复制与p53状态无关,即靶细胞的p53状态并不能可靠地预测ONYX-015的复制或细胞杀伤能力 | 5c |
| 基础研究[ | ONYX-015 | 正常细胞与肿瘤细胞之间的RNA输出差异,而非p53表达状态,决定了ONYX-015的特异性溶瘤 | 5c |
| Ⅱ期临床研究[ | H101 | 未发现p53异常与H101的临床疗效明显相关 | 2d |
| 类实验性研究[ | H101 | H101治疗p53突变型患者的有效率显著高于p53无突变型患者(72.3% vs 36.3%,P<0.05),但H101对p53无突变型肿瘤患者也有一定疗效 | 2d |
"
| 研究类型 | 抗病毒药物 | 溶瘤病毒 | 主要结果 | 证据级别 |
|---|---|---|---|---|
| 回顾性研究[ | 恩替卡韦、拉米夫定和阿德福韦酯 | 腺病毒H101 | 未发现抗病毒治疗在肿瘤应答或OS和PFS方面对H101疗效有显著影响 | 3c |
| 回顾性研究[ | 腺病毒H101 | 抗病毒治疗是HCC患者的独立预后因素,并提出H101联合抗病毒治疗可能提高TACE治疗HCC的疗效,但尚需进一步研究确认 | 3c | |
| 基础研究[ | IFN-α | 腺病毒SG600-IL-24 | IFN-α联合SG600-IL-24相比IFN-α或SG600-IL-24单药治疗,可显著延长HCC小鼠的中位生存时间,降低肿瘤体积,采取联合治疗的8只小鼠中,有3只长期存活,提示IFN-α可能增加溶瘤腺病毒SG600-IL-24的抗肿瘤活性 | 5c |
| 基础研究[ | ① 用于治疗临床乙型肝炎病毒感染的一线药物,如口服核苷类似物恩替卡韦、拉米夫定、阿德福韦、特比夫定和替诺福韦;② 欧洲和美国推荐用于治疗丙型肝炎病毒感染的新药,如达卡他韦、特拉匹韦和索非布韦;③ 广谱抗病毒药物,如IFN-α和利巴韦林 | 天然甲病毒M1 | 除IFN-α能够抑制M1病毒的溶瘤作用,上述的其他抗病毒试剂均不会抑制M1诱导的溶瘤作用 | 5c |
| 基础研究[ | IFN-α | 单纯疱疹病毒G207和ONCR-177 | 在IFN-α存在的情况下,ICP34.5缺失的G207的复制能力被消除或被抑制了135倍,而ICP34.5保留的ONCR-177仅被适度抑制了4.5 ~ 6.0倍,提示ICP34.5保留可能是单纯疱疹病毒在IFN-α存在的情况下进行有效复制的关键因素 | 5c |
"
"
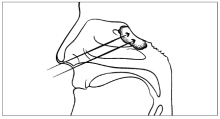
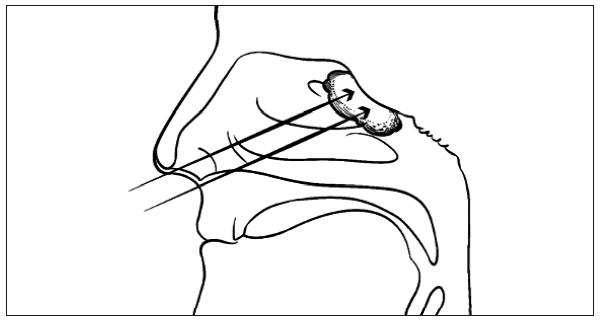
| 给药方式 | 瘤内注射 | 静脉注射 |
|---|---|---|
| 优点 | 更好地控制病毒的分布,增加肿瘤内的病毒浓度,避免系统体液免疫反应的抗体中和,从而获得更好的疗效[ | 操作方便,可以将溶瘤病毒递送至深部肿瘤部位或多个转移部位,因此,对于不适合瘤内注射的转移性肿瘤或血液系统恶性肿瘤患者,静脉注射是一种有潜力的给药方式[ |
| 缺点 | 难以接近深层内脏肿瘤或位于中枢神经系统内的肿瘤,且需要为每例患者量身定制给药体积和注射部位,特别是需要重复给药时,操作较为复杂,对医务人员的技术要求较高[ | 溶瘤病毒经过血液稀释及血清中抗体中和杀伤,其在肿瘤组织中较难达到有效浓度,因此对溶瘤病毒的剂量要求更高[ |
"
| 研究类型 | 干预措施 | 常见不良反应 | 证据级别 |
|---|---|---|---|
| Ⅲ期临床试验b[ | 瘤内注射H101联合化疗治疗头颈部及食管鳞癌 | 白细胞下降(59.8%)、轻~中度发热(45.7%)、粒细胞下降(42.4%)、注射局部反应(28.3%) | 1c |
| Ⅰ期临床试验[ | 瘤内注射H101治疗恶性肿瘤 | 注射部位疼痛(60.0%)、流感样症状(53.3%)、发热(33.3%)、恶心呕吐(20.0%) | 2d |
| Ⅱ期临床试验[ | 瘤内注射H101联合化疗治疗恶性肿瘤 | 白细胞减少(49.1%)、恶性呕吐(34.0%)、发热(30.2%)、流感样症状(28.3%)、注射部位疼痛(26.4%) | 2c |
"
| 编号 | 陈述 | 推荐强度 | 同意率 | 不同意率 | 不确定率 |
|---|---|---|---|---|---|
| 基因重组溶瘤腺病毒的适用范围 | |||||
| 1 | 对于无法切除或术后复发转移的鼻咽癌患者,初始治疗可选择H101瘤内注射联合顺铂和5-FU | 强推荐 | 95.3% | 2.4% | 2.4% |
| 2 | 对于无法切除、Child-Pugh肝功能分级为A或B级、无肝外转移的HCC患者,初始治疗可考虑肝动脉注射H101联合TACE | 推荐 | 88.4% | 2.3% | 9.3% |
| 国外已获批上市溶瘤病毒及其适应证 | |||||
| 3 | 对于无法切除的Ⅲ期黑色素瘤,初始治疗可选择病灶内注射T-VEC | 强推荐 | 97.6% | 1.2% | 1.2% |
| 4 | 对于不可切除、BRAF野生型、Ⅲb ~ Ⅳ期黑色素瘤,二线或后续治疗可考虑伊匹单抗联合病灶内注射T-VEC | 强推荐 | 98.8% | 0.0% | 1.2% |
| 5 | 对于有残余肿瘤或复发的恶性胶质瘤患者,可考虑颅内注射单纯疱疹病毒G47△ | 强推荐 | 91.1% | 2.5% | 6.3% |
| 溶瘤病毒药物未来的发展趋势 | |||||
| 6 | 溶瘤病毒与化疗、放疗、靶向治疗和(或)免疫治疗联合可能具有协同抗肿瘤效应,在恶性肿瘤,尤其在难治性肿瘤患者中具有较大潜力,建议开展注册临床研究以拓展溶瘤病毒的治疗模式 | 强推荐 | 97.0% | 1.5% | 1.5% |
| 7 | 不同疗法的组合方式、适用患者的选择标准、给药剂量、给药顺序及时间间隔等均可能影响溶瘤病毒的抗肿瘤活性,建议开展注册研究以深入探讨这些问题 | 强推荐 | 98.5% | 0.0% | 1.5% |
| 8 | 临床前研究及早期临床试验证实溶瘤病毒疗法在结直肠癌肝转移患者中的安全性良好,且表现出初步的抗肿瘤活性,建议开展注册研究以拓展溶瘤病毒在肝转移癌患者中的适应证 | 强推荐 | 98.5% | 0.0% | 1.5% |
| 9 | 溶瘤病毒疗法治疗恶性胶质瘤的安全性已得到大量临床前及早期临床试验证实,建议开展注册研究以进一步验证溶瘤病毒疗法在恶性胶质瘤患者中的抗肿瘤疗效 | 强推荐 | 97.0% | 0.0% | 3.0% |
| 10 | 溶瘤病毒疗法在恶性胸腹腔积液患者中的治疗潜力已在一些动物研究及临床研究中得到证实,建议开展大样本、高质量的临床研究以拓展溶瘤病毒在恶性胸腹腔积液患者中的适应证 | 强推荐 | 93.9% | 0.0% | 6.1% |
| 11 | 临床研究显示,溶瘤病毒疗法在胰腺癌患者中具有良好的安全性和疗效,建议开展大样本、高质量的临床研究以拓展溶瘤病毒在胰腺癌患者中的适应证 | 强推荐 | 93.9% | 0.0% | 6.1% |
| 12 | 鉴于溶瘤病毒胸腔注射的可操作性及其在MPM中表现出的抗肿瘤潜力,建议在MPM尤其是CDKN2A纯合缺失的患者中开展溶瘤病毒治疗研究 | 强推荐 | 93.9% | 0.0% | 6.1% |
| 13 | 临床前研究发现,溶瘤病毒可特异性杀伤子宫颈癌细胞,也可以作为一个或多个治疗基因的载体,增强抗肿瘤疗效,或与放疗等常规疗法协同抗肿瘤,溶瘤病毒可能是未来治疗子宫颈癌的新型疗法,建议在对现有治疗模式耐药的子宫颈癌患者中开展溶瘤病毒相关临床研究 | 强推荐 | 91.5% | 0.0% | 8.5% |
| 基因重组溶瘤腺病毒的使用方法 | |||||
| 14 | 使用基因重组溶瘤腺病毒前,建议对患者的以下情况进行评估:① 一般情况评估:年龄、体能状态评分、是否处于妊娠期或哺乳期、重要脏器功能;② 病史评估:有无同类生物制剂过敏史、有无恶性血液系统疾病、有无未经控制的活动性感染、有无免疫缺陷或免疫功能低下;③ 用药史评估:过去4周是否使用过抗病毒药物、免疫抑制剂或肾上腺糖皮质激素药物;④ 既往治疗方案评估:是否接受过其他抗肿瘤治疗,如手术、放疗、化疗及生物治疗等;⑤ 影像学评估:病灶数量、大小、位置、有无转移等 | 推荐 | 89.5% | 0.0% | 10.5% |
| 15 | 计划应用基因重组溶瘤腺病毒治疗的患者应至少满足以下要求:① 经影像学、细胞学或病理组织学检查确诊为恶性肿瘤;② 年龄18 ~ 75岁;③ 肝肾功能良好;④ 体力状况0 ~ 2级(WHO分级);⑤ 无明显骨髓抑制;⑥ 签署知情同意书 | 推荐 | 83.1% | 0.0% | 16.9% |
| 16 | p53与E1B-55K缺陷型腺病毒的关系尚存在争议,对于计划使用H101治疗的患者,可不进行p53基因检测 | 未达成 共识 | 73.8% | 4.6% | 21.5% |
| 17 | 以下情况应慎用或禁用基因重组溶瘤腺病毒类药物:① 有同类生物制剂过敏史者;② 恶性血液系统疾病者;③ 有未经控制的活动性感染者;④ 正在使用抗病毒药物或大剂量肾上腺糖皮质激素类药物者;⑤ 免疫缺陷和免疫抑制者;⑥ 哺乳、妊娠期妇女 | 强推荐 | 93.9% | 0.0% | 6.1% |
| 18 | 目前尚无证据表明抗病毒药物与基因重组溶瘤腺病毒药物有任何潜在的相互作用,对于计划使用H101治疗的HCC患者,可继续使用抗病毒药物(恩替卡韦、拉米夫定和阿德福韦酯),其他情况下,应谨慎使用 | 强推荐 | 97.0% | 3.0% | 0.0% |
| 19 | 溶瘤病毒的给药途径包括瘤内注射、静脉注射、肝动脉注射、胸腹腔内注射等,其中瘤内注射与静脉注射各有利弊,临床医师应根据病毒类型、肿瘤部位和治疗目的选择合适的给药途径 | 强推荐 | 98.5% | 0.0% | 1.5% |
| 20 | 对于易通过临床或影像学方法测量,且适合直接注射或超声引导注射的肿瘤病灶,推荐首选瘤内注射的方式给药,建议选取血供丰富的地方注射,避开大血管 | 未达成 共识 | 69.8% | 1.2% | 29.1% |
| 21 | 对于不适合进行瘤内注射的患者,在充分考虑静脉注射溶瘤病毒的风险和益处后,可尝试静脉注射 | 未达成 共识 | 66.2% | 9.2% | 24.6% |
| 22 | 在充分考虑溶瘤病毒药物的可及性、安全性、有效性及操作可行性后,也可考虑其他给药方式,如肝动脉注射、胸腹腔内注射 | 强推荐 | 94.1% | 1.2% | 4.7% |
| 23 | 建议根据肿瘤体积大小及病灶数量决定H101的剂量 | 强推荐 | 95.3% | 1.2% | 3.5% |
| 24 | 对于接受H101治疗的鼻咽癌患者,建议H101与化疗药物同步使用,直接瘤内注射,每天1次,每次注射0.5×1012 ~ 1.5×1012 vp,连续5 d,21 d为1个周期 | 未达成 共识 | 64.7% | 1.2% | 34.1% |
| 25 | 对于接受TACE联合H101治疗的HCC患者,建议在注射化疗剂之前,将含有1.0×1012 vp的10 mL 0.9%氯化钠溶液通过导管全部注入供应肿瘤的肝动脉 | 未达成 共识 | 68.2% | 1.2% | 30.6% |
| 2826 | 溶瘤病毒应低温储存和运输,其中H101的储存和运输温度为-20 ℃,T-VEC的储存和运输温度为-70 ℃,T-VEC应避光保存 | 强推荐 | 97.6% | 2.4% | 0.0% |
| 27 | 给药前应先将溶瘤病毒药物置于室温下解冻,直至药物转化为液态。使用过程中应避免反复冻融或在室温下放置过久而导致药效下降 | 强推荐 | 100.0% | 0.0% | 0.0% |
| 28 | 使用溶瘤病毒前,应对患者及其家属以及相关医护人员进行药物使用说明及防护知识教育 | 强推荐 | 100.0% | 0.0% | 0.0% |
| 29 | 医护人员及其家属、孕妇和新生儿应避免直接接触患者的病变注射处、敷料或体液;免疫功能低下或处于妊娠期的医护人员应避免制备或注射溶瘤病毒;患者应避免触碰或抓挠注射部位及其封闭敷料 | 强推荐 | 98.5% | 0.0% | 1.5% |
| 30 | 在制备和注射溶瘤病毒时,医护人员应穿戴个人防护装备(如工作服、安全眼镜、口罩和手套),避免溶瘤病毒药物接触到皮肤、眼睛和黏膜,若溅入眼睛或黏膜,应立即使用清水反复冲洗;若接触皮肤或被针头刺伤,应立即用75%乙醇溶液擦拭,再用清水彻底清洗 | 强推荐 | 96.9% | 0.0% | 3.1% |
| 31 | 建议将所有可能接触过溶瘤病毒药物的材料(如药瓶、注射器、手套、口罩、敷料)作为生物危险废物进行处置 | 强推荐 | 100.0% | 0.0% | 0.0% |
| 32 | 建议参考美国国立癌症研究所发布的最新版常见不良反应术语评定标准对基因重组溶瘤腺病毒相关不良反应进行评价和分级 | 强推荐 | 98.8% | 0.0% | 1.2% |
| 33 | 对于1或2级不良反应,建议对症处理,并继续使用基因重组溶瘤腺病毒治疗,同时密切监测病情严重程度的变化 | 强推荐 | 98.8% | 0.0% | 1.2% |
| 34 | 对于3级及以上不良反应,建议紧急对症处理,并停止基因重组溶瘤腺病毒治疗 | 强推荐 | 97.6% | 0.0% | 2.4% |
| 随访与疗效评估 | |||||
| 35 | 对于使用H101治疗的鼻咽癌患者,建议在治疗后的4 ~ 6周时进行复查评估,随后根据情况可间隔1 ~ 3个月复查 | 强推荐 | 98.8% | 0.0% | 1.2% |
| 36 | 对于使用H101治疗的鼻咽癌患者,建议随访以下内容:纤维鼻咽镜或鼻内镜评估、注射部位的CT或MRI、转移部位的B超、脏器功能(包括肾功能、听力、甲状腺功能)、免疫功能、口腔科检查。其他检查还包括心脏、眼部、关节损害和其他晚期不良反应如继发的恶性肿瘤等相关检查 | 强推荐 | 100.0% | 0.0% | 0.0% |
| 37 | 对于使用H101治疗的HCC患者,建议在治疗后的4 ~ 6周时进行复查评估,随后根据情况可间隔1 ~ 3个月随访1次 | 强推荐 | 97.6% | 1.2% | 1.2% |
| 38 | 对于使用H101治疗的HCC患者,建议随访以下内容:甲胎蛋白、肝肾功能检测、影像学检查(注射部位的CT或MRI,也可视情况进行胸部X线、腹部超声、肝脏超声造影或肿瘤负荷评分) | 强推荐 | 97.6% | 1.2% | 1.2% |
| 39 | 对于采取局部注射溶瘤病毒的患者,建议同时评估注射病灶与非注射病灶 | 强推荐 | 100.0% | 0.0% | 0.0% |
"
| 瘤种 | 溶瘤病毒类型 | 病毒名称 | 临床分期 | 联合干预方案 | 注册号 |
|---|---|---|---|---|---|
| 恶性胸腹水 | 腺病毒 | H101 | Ⅱ期 | 单药 | NCT04771676 |
| 肝癌 | 腺病毒 | H101 | Ⅲ期 | 联合化疗 | NCT03780049 |
| 肝癌 | 单纯疱疹病毒 | T-VEC | Ⅱ期 | 联合免疫治疗 | NCT02509507 |
| 肝癌 | 痘病毒 | Pexa-Vec | Ⅲ期 | 联合靶向治疗 | NCT02562755 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅱ期 | 联合化疗 | NCT04427306 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅱ期 | 联合免疫治疗 | NCT04068181 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅱ期 | 联合化疗 | NCT03972046 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅰ期 | 联合免疫治疗 | NCT03747744 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅱ期 | 联合免疫治疗 | NCT02965716 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅲ期 | 联合免疫治疗 | NCT02263508 |
| 黑色素瘤 | 单纯疱疹病毒 | T-VEC | Ⅲ期 | 单药 | NCT01368276 |
| 头颈部癌 | 单纯疱疹病毒 | T-VEC | Ⅰ期 | 联合免疫治疗 | NCT02626000 |
| 头颈部癌 | 呼肠孤病毒 | Pelareorep | Ⅲ期 | 联合化疗 | NCT01166542 |
| 胰腺癌 | 单纯疱疹病毒 | T-VEC | Ⅰ期 | 单药 | NCT03086642 |
| 胰腺癌 | 单纯疱疹病毒 | T-VEC | Ⅰ期 | 单药 | NCT00402025 |
| 食管癌 | 腺病毒 | OBP-301 | Ⅰ期 | 联合免疫治疗 | NCT03172819 |
| 胶质瘤 | 腺病毒 | DNX-2401 | Ⅰ期 | 联合手术 | NCT03896568 |
| 神经内分泌瘤 | 腺病毒 | AdVince | Ⅰ/Ⅱa | 单药 | NCT02749331 |
| 结直肠癌,卵巢癌 | 腺病毒 | ONCOS-102 | Ⅰ/Ⅱ | 联合免疫治疗 | NCT02963831 |
| 卵巢癌 | 腺病毒 | EnAd | Ⅰ | 单药 | NCT02028117 |
| 肉瘤 | 单纯疱疹病毒 | T-VEC | Ⅱ | 联合免疫治疗 | NCT03069378 |
| 乳腺癌 | 单纯疱疹病毒 | T-VEC | Ⅰ/Ⅱ | 联合化疗 | NCT02779855 |
| 卵巢癌,输卵管癌,腹膜转移癌 | 牛痘病毒 | GL-ONC1 | Ⅰb/Ⅱ | 单药 | NCT02759588 |
| 尿路上皮癌 | 麻疹病毒 | MV-NIS | Ⅰ | 联合手术 | NCT03171493 |
| 非小细胞肺癌 | 犬腺病毒 | CVA21 | Ⅰ | 联合免疫治疗 | NCT02824965 |
| 多发性骨髓瘤 | 麻疹病毒 | MV-NIS | Ⅱ | 联合化疗 | NCT02192775 |
| [1] |
HEMMINKI O, DOS SANTOS J M, HEMMINKI A. Oncolytic viruses for cancer immunotherapy[J]. J Hematol Oncol, 2020, 13(1): 84.
doi: 10.1186/s13045-020-00922-1 |
| [2] |
JHAWAR S R, THANDONI A, BOMMAREDDY P K, et al. Oncolytic viruses-natural and genetically engineered cancer immunotherapies[J]. Front Oncol, 2017, 7: 202.
doi: 10.3389/fonc.2017.00202 pmid: 28955655 |
| [3] |
SHAO X Y, WANG X K, GUO X L, et al. STAT3 contributes to oncolytic Newcastle disease virus-induced immunogenic cell death in melanoma cells[J]. Front Oncol, 2019, 9: 436.
doi: 10.3389/fonc.2019.00436 pmid: 31192135 |
| [4] |
WANG X K, SHAO X Y, GU L, et al. Targeting STAT3 enhances NDV-induced immunogenic cell death in prostate cancer cells[J]. J Cell Mol Med, 2020, 24(7): 4286-4297.
doi: 10.1111/jcmm.15089 pmid: 32100392 |
| [5] |
BREITBACH C J, ARULANANDAM R, DE SILVA N, et al. Oncolytic vaccinia virus disrupts tumor-associated vasculature in humans[J]. Cancer Res, 2013, 73(4): 1265-1275.
doi: 10.1158/0008-5472.CAN-12-2687 pmid: 23393196 |
| [6] |
COOK M, CHAUHAN A. Clinical application of oncolytic viruses: a systematic review[J]. Int J Mol Sci, 2020, 21(20): 7505.
doi: 10.3390/ijms21207505 |
| [7] |
LI Y W, SHEN Y N, TANG T Y, et al. Oncolytic virus combined with traditional treatment versus traditional treatment alone in patients with cancer: a meta-analysis[J]. Int J Clin Oncol, 2020, 25(11): 1901-1913.
doi: 10.1007/s10147-020-01760-4 |
| [8] |
LI Z B, JIANG Z J, ZHANG Y X, et al. Efficacy and safety of oncolytic viruses in randomized controlled trials: a systematic review and meta-analysis[J]. Cancers (Basel), 2020, 12(6): 1416.
doi: 10.3390/cancers12061416 |
| [9] |
GARBER K. China approves world’s first oncolytic virus therapy for cancer treatment[J]. J Natl Cancer Inst, 2006, 98(5): 298-300.
doi: 10.1093/jnci/djj111 |
| [10] | 许青, 陆舜, 朱蕙燕, 等. 溶瘤病毒治疗恶性肿瘤临床应用上海专家共识(2021年版)[J]. 中国癌症杂志, 2021, 31(3): 231-240. |
| XU Q, LU S, ZHU H Y, et al. Shanghai expert consensus on clinical application of oncolytic virus in the treatment of malignant tumors (2021 edition)[J]. China Oncol, 2021, 31(3): 231-240. | |
| [11] |
HASSETT M J, SOMERFIELD M R, BAKER E R, et al. Management of male breast cancer: ASCO guideline[J]. J Clin Oncol, 2020, 38(16): 1849-1863.
doi: 10.1200/JCO.19.03120 pmid: 32058842 |
| [12] | 王春青, 胡雁. JBI证据预分级及证据推荐级别系统(2014版)[J]. 护士进修杂志, 2015, 30(11): 964-967. |
| WANG C Q, HU Y. JBI evidence pre-classification and evidence rank system (2014 edition)[J]. J Nurses Train, 2015, 30(11): 964-967. | |
| [13] |
BISCHOFF J R, KIRN D H, WILLIAMS A, et al. An adenovirus mutant that replicates selectively in p53-deficient human tumor cells[J]. Science, 1996, 274(5286): 373-376.
doi: 10.1126/science.274.5286.373 pmid: 8832876 |
| [14] | 蒋泓, 刘芳, 严爱芬, 等. 溶瘤病毒的肿瘤治疗作用研究[J]. 佛山科学技术学院学报(自然科学版), 2013, 31(2): 1-6. |
| JIANG H, LIU F, YAN A F, et al. The application of oncolytic virus to cancer therapy[J]. J Foshan Univ Nat Sci Ed, 2013, 31(2): 1-6. | |
| [15] | 夏忠军, 常建华, 张力, 等. 基因工程腺病毒(H101)瘤内注射联合化疗治疗头颈部及食管鳞癌的Ⅲ期临床研究[J]. 癌症, 2004, 23(12): 1666-1670. |
| XIA Z J, CHANG J H, ZHANG L, et al. Phase Ⅲ randomized clinical trial of intratumoral injection of E1B gene-deleted adenovirus (H101) combined with cisplatin-based chemotherapy in treating squamous cell cancer of head and neck or esophagus[J]. Chin J Cancer, 2004, 23(12): 1666-1670. | |
| [16] | 陆永奎, 胡晓桦, 黎福祥, 等. 基因工程腺病毒(H101)瘤内注射联合化疗治疗鼻咽癌的疗效观察[J]. 中国肿瘤临床, 2005, 32(19): 1096-1099. |
| LU Y K, HU X H, LI F X, et al. Clinical observation of intratumoral injection of E1B gene-deleted adenovirus (H101) combined with chemotherapy in treatment of nasopharyngeal carcinoma[J]. Chin J Clin Oncol, 2005, 32(19): 1096-1099. | |
| [17] | 中国医师协会介入医师分会. 中国肝细胞癌经动脉化疗栓塞治疗(TACE)临床实践指南[J]. 中华肝脏病杂志, 2019, 27(3)1117-1126 |
| Interventional Physicians Branch of Chinese Medical Association. Chinese clinical practice guidelines for transarterial chemoembolization of hepatocellular carcinoma[J]. Chin J Hepatol, 2019, 27(3)1117-1126 | |
| [18] |
LIN X J, LI Q J, LAO X M, et al. Transarterial injection of recombinant human type-5 adenovirus H101 in combination with transarterial chemoembolization (TACE) improves overall and progressive-free survival in unresectable hepatocellular carcinoma (HCC)[J]. BMC Cancer, 2015, 15: 707.
doi: 10.1186/s12885-015-1715-x |
| [19] |
HE C B, ZHANG Y, LIN X J. Increased overall survival and decreased cancer-specific mortality in patients with hepatocellular carcinoma treated by transarterial chemoembolization and human adenovirus type-5 combination therapy: a competing risk analysis[J]. J Gastrointest Surg, 2018, 22(6): 989-997.
doi: 10.1007/s11605-018-3703-3 pmid: 29435900 |
| [20] | 陆吉麟, 张浩, 石伟, 等. 重组人5型腺病毒注射液局部瘤内注射治疗晚期肝癌的临床研究[J]. 中国现代医师, 2021, 59(12): 10-15. |
| LU J L, ZHANG H, SHI W, et al. Clinical research on topical intratumoral injection of recombinant human adenovirus type 5 in the treatment of advanced liver cancer[J]. China Mod Dr, 2021, 59(12): 10-15. | |
| [21] | XIE A Q, XIA F, PEI J, et al. Advanced hepatocellular carcinoma treated by radiofrequency ablation combined with oncolytic virus and anti-PD-1 antibody therapy: a case report and literature review[J]. J Int Med Res, 2021, 49(9): 3000605211044596. |
| [22] |
ANDTBACKA R H, KAUFMAN H L, COLLICHIO F, et al. Talimogene laherparepvec improves durable response rate in patients with advanced melanoma[J]. J Clin Oncol, 2015, 33(25): 2780-2788.
doi: 10.1200/JCO.2014.58.3377 pmid: 26014293 |
| [23] |
TODO T, ITO H, INO Y, et al. Intratumoral oncolytic herpes virus G47∆ for residual or recurrent glioblastoma: a phase 2 trial[J]. Nat Med, 2022, 28(8): 1630-1639.
doi: 10.1038/s41591-022-01897-x pmid: 35864254 |
| [24] | RASA A, ALBERTS P. Oncolytic virus preclinical toxicology studies[J]. J Appl Toxicol, 2022. |
| [25] | 徐雪丽, 张伟, 胡又佳. 溶瘤病毒在肿瘤治疗中的研究进展[J]. 世界临床药物, 2014, 35(11): 710-716. |
| XU X L, ZHANG W, HU Y J. Research progress of oncolysis virus on tumor therapy[J]. World Clin Drugs, 2014, 35(11): 710-716. | |
| [26] |
QUINN C, MA Q F, KUDLAC A, et al. Indirect treatment comparison of talimogene laherparepvec compared with ipilimumab and vemurafenib for the treatment of patients with metastatic melanoma[J]. Adv Ther, 2016, 33(4): 643-657.
doi: 10.1007/s12325-016-0313-x pmid: 26979173 |
| [27] |
CHESNEY J, PUZANOV I, COLLICHIO F, et al. Randomized, open-label phase Ⅱ study evaluating the efficacy and safety of talimogene laherparepvec in combination with ipilimumab versus ipilimumab alone in patients with advanced, unresectable melanoma[J]. J Clin Oncol, 2018, 36(17): 1658-1667.
doi: 10.1200/JCO.2017.73.7379 |
| [28] | National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology (NCCN guidelines®) non-small cell lung cancer (version 3, 2018)[EB/OL]. (2021-06-06)[2022-12-01]. www.nccn.org/patients. |
| [29] |
TODO T, MARTUZA R L, RABKIN S D, et al. Oncolytic herpes simplex virus vector with enhanced MHC class Ⅰ presentation and tumor cell killing[J]. Proc Natl Acad Sci U S A, 2001, 98(11): 6396-6401.
doi: 10.1073/pnas.101136398 |
| [30] | Brain cancer. SNO 2019: the oncolytic herpes virus G47∆ may lead to a potential cure of malignant glioma[EB/OL]. (2019-02-02)[2022-12-10].https://www.practiceupdate.com/content/sno-2019-the-oncolytic-herpes-virus-g47-may-lead-to-a-potential-cure-of-malignant-glioma/92833. |
| [31] |
LIU Y, CAI J, LIU W F, et al. Intravenous injection of the oncolytic virus M1 awakens antitumor T cells and overcomes resistance to checkpoint blockade[J]. Cell Death Dis, 2020, 11(12): 1062.
doi: 10.1038/s41419-020-03285-0 pmid: 33311488 |
| [32] |
ROJAS J J, SAMPATH P, HOU W Z, et al. Defining effective combinations of immune checkpoint blockade and oncolytic virotherapy[J]. Clin Cancer Res, 2015, 21(24): 5543-5551.
doi: 10.1158/1078-0432.CCR-14-2009 pmid: 26187615 |
| [33] |
FEND L, YAMAZAKI T, REMY C, et al. Immune checkpoint blockade, immunogenic chemotherapy or IFN-α blockade boost the local and abscopal effects of oncolytic virotherapy[J]. Cancer Res, 2017, 77(15): 4146-4157.
doi: 10.1158/0008-5472.CAN-16-2165 pmid: 28536278 |
| [34] |
XIE R Y, BI X G, SHANG B Q, et al. Efficacy and safety of oncolytic viruses in advanced or metastatic cancer: a network meta-analysis[J]. Virol J, 2021, 18(1): 158.
doi: 10.1186/s12985-021-01630-z pmid: 34332591 |
| [35] |
BERNSTEIN V, ELLARD S L, DENT S F, et al. A randomized phase Ⅱ study of weekly paclitaxel with or without pelareorep in patients with metastatic breast cancer: final analysis of Canadian Cancer Trials Group IND.213[J]. Breast Cancer Res Treat, 2018, 167(2): 485-493.
doi: 10.1007/s10549-017-4538-4 |
| [36] |
RIBAS A, CHESNEY J, LONG G V, et al. 1037O MASTERKEY-265: a phase Ⅲ, randomized, placebo (Pbo)-controlled study of talimogene laherparepvec (T) plus pembrolizumab (P) for unresectable stage ⅢB-ⅣM1c melanoma (MEL)[J]. Ann Oncol, 2021, 32: S868-S869.
doi: 10.1016/j.annonc.2021.08.1422 |
| [37] |
RIBAS A, DUMMER R, PUZANOV I, et al. Oncolytic virotherapy promotes intratumoral T cell infiltration and improves anti-PD-1 immunotherapy[J]. Cell, 2018, 174(4): 1031-1032.
doi: S0092-8674(18)30963-2 pmid: 30096300 |
| [38] |
GUO J, CUI C L, WANG X, et al. A phase Ⅰb clinical trial of anti-PD-1 ab (toripalimab) plus intralesional injection of OrienX010 in stage melanoma with liver metastases[J]. J Clin Oncol, 2021, 39(15_suppl): 9559.
doi: 10.1200/JCO.2021.39.15_suppl.9559 |
| [39] |
WANG X, CUI C L, SI L, et al. A phase Ⅰb clinical trial of neoadjuvant OrienX010, an oncolytic virus, in combination with toripalimab in patients with resectable stage Ⅲb to stage ⅣM1a acral melanoma[J]. J Clin Oncol, 2021, 39(15_suppl): 9570.
doi: 10.1200/JCO.2021.39.15_suppl.9570 |
| [40] | ZHAO H X, GUO X L, LIU Z Q, et al. Recombinant human adenovirus 5 injection plus toripalimab therapy in patients with advanced and refractory melanoma: a single arm, single-center, prospective study[J]. J Clin Oncol, 2022, 40(16_suppl): e21503. |
| [41] |
ZHANG Q N, LI Y, ZHAO Q, et al. Recombinant human adenovirus type 5 (Oncorine) reverses resistance to immune checkpoint inhibitor in a patient with recurrent non-small cell lung cancer: a case report[J]. Thorac Cancer, 2021, 12(10): 1617-1619.
doi: 10.1111/tca.v12.10 |
| [42] |
HE Y, CHEN J H, ZHU Z Z, et al. H101 treatment of hepatic metastasis of colorectal cancer with recombinant human adenovirus 5 injection: a phase Ⅰ clinical trial-TROJAN 021[J]. J Clin Oncol, 2021, 39(15_suppl): 3605-3605.
doi: 10.1200/JCO.2021.39.15_suppl.3605 |
| [43] |
GEEVARGHESE S K, GELLER D A, DE HAAN H A, et al. Phase Ⅰ/Ⅱ study of oncolytic herpes simplex virus NV1020 in patients with extensively pretreated refractory colorectal cancer metastatic to the liver[J]. Hum Gene Ther, 2010, 21(9): 1119-1128.
doi: 10.1089/hum.2010.020 |
| [44] |
CAFFERATA E G, MACCIÓ D R, LOPEZ M V, et al. A novel A33 promoter-based conditionally replicative adenovirus suppresses tumor growth and eradicates hepatic metastases in human colon cancer models[J]. Clin Cancer Res, 2009, 15(9): 3037-3049.
doi: 10.1158/1078-0432.CCR-08-1161 pmid: 19336523 |
| [45] |
CHIOCCA E A, ABBED K M, TATTER S, et al. A phase I open-label, dose-escalation, multi-institutional trial of injection with an E1B-attenuated adenovirus, ONYX-015, into the peritumoral region of recurrent malignant gliomas, in the adjuvant setting[J]. Mol Ther, 2004, 10(5): 958-966.
doi: 10.1016/j.ymthe.2004.07.021 pmid: 15509513 |
| [46] | 米中波, 焦保华. 重组人5型腺病毒术中瘤腔内注射治疗脑胶质瘤的安全性研究[J]. 河北医药, 2009, 31(14): 1760-1761. |
| MI Z B, JIAO B H. Study on the safety of intra-operative injection of recombinant human adenovirus type 5 in the treatment of glioma[J]. Hebei Med J, 2009, 31(14): 1760-1761. | |
| [47] |
LANG F F, CONRAD C, GOMEZ-MANZANO C, et al. Phase Ⅰ study of DNX-2401 (delta-24-RGD) oncolytic adenovirus: replication and immunotherapeutic effects in recurrent malignant glioma[J]. J Clin Oncol, 2018, 36(14): 1419-1427.
doi: 10.1200/JCO.2017.75.8219 |
| [48] | 杨帆, 卢斌, 胡春燕, 等. 胸腔内注射重组人5型腺病毒治疗晚期肺癌恶性胸腔积液的疗效观察[J]. 实用医学杂志, 2013, 29(17): 2885-2886. |
| YANG F, LU B, HU C Y, et al. Therapeutic effect of intrathoracic injection of recombinant human adenovirus type 5 on malignant pleural effusion of advanced lung cancer[J]. J Pract Med, 2013, 29(17): 2885-2886. | |
| [49] | 王维, 李枋霏, 肖彩芝, 等. 攻癌利水散外敷联合重组人5型腺病毒注射液胸腔内灌注治疗肺癌恶性胸水的临床疗效[J]. 中国老年学杂志, 2018, 38(21): 5184-5186. |
| WANG W, LI F F, XIAO C Z, et al. Clinical efficacy of external application of Gongailishui Powder combined with intrathoracic perfusion of recombinant human adenovirus type 5 injection in the treatment of malignant pleural effusion of lung cancer[J]. Chin J Gerontol, 2018, 38(21): 5184-5186. | |
| [50] |
ZHANG Y L, QIAN L, CHEN K, et al. Intraperitoneal oncolytic virotherapy for patients with malignant ascites: characterization of clinical efficacy and antitumor immune response[J]. Mol Ther Oncolytics, 2022, 25: 31-42.
doi: 10.1016/j.omto.2022.03.003 |
| [51] | LIU H L, CHEN J. Oncolytic virus as an agent for the treatment of malignant ascites[J]. Cancer Biother Radiopharm, 2009, 24(1): 99-102. |
| [52] |
ZHOU Y, WEN F, ZHANG P F, et al. Vesicular stomatitis virus is a potent agent for the treatment of malignant ascites[J]. Oncol Rep, 2016, 35(3): 1573-1581.
doi: 10.3892/or.2015.4522 pmid: 26707610 |
| [53] | HECHT J R, BEDFORD R, ABBRUZZESE J L, et al. A phase Ⅰ/Ⅱ trial of intratumoral endoscopic ultrasound injection of ONYX-015 with intravenous gemcitabine in unresectable pancreatic carcinoma[J]. Clin Cancer Res, 2003, 9(2): 555-561. |
| [54] | 朱颖炜, 龚镭, 吴高珏, 等. 超声内镜引导下瘤体内注射H101治疗胰腺癌疗效分析[J]. 南京医科大学学报(自然科学版), 2016, 36(10): 1166-1169. |
| ZHU Y W, GONG L, WU G J, et al. Therapeutic effects analysis of tumor injection of H101 guided by endoscopic ultrasonography for patients with pancreatic carcinoma[J]. J Nanjing Med Univ Nat Sci, 2016, 36(10): 1166-1169. | |
| [55] |
MAHALINGAM D, WILKINSON G A, ENG K H, et al. Pembrolizumab in combination with the oncolytic virus pelareorep and chemotherapy in patients with advanced pancreatic adenocarcinoma: a phase Ⅰb study[J]. Clin Cancer Res, 2020, 26(1): 71-81.
doi: 10.1158/1078-0432.CCR-19-2078 |
| [56] |
HIROOKA Y, KASUYA H, ISHIKAWA T, et al. A phase Ⅰ clinical trial of EUS-guided intratumoral injection of the oncolytic virus, HF10 for unresectable locally advanced pancreatic cancer[J]. BMC Cancer, 2018, 18(1): 596.
doi: 10.1186/s12885-018-4453-z |
| [57] |
DANSON S J, CONNER J, EDWARDS J G, et al. Oncolytic herpesvirus therapy for mesothelioma-a phase Ⅰ/Ⅱa trial of intrapleural administration of HSV1716[J]. Lung Cancer, 2020, 150: 145-151.
doi: 10.1016/j.lungcan.2020.10.007 |
| [58] |
DELAUNAY T, ACHARD C, BOISGERAULT N, et al. Frequent homozygous deletions of type Ⅰ interferon genes in pleural mesothelioma confer sensitivity to oncolytic measles virus[J]. J Thorac Oncol, 2020, 15(5): 827-842.
doi: 10.1016/j.jtho.2019.12.128 |
| [59] |
ZHANG J, ZHANG Q Y, LIU Z, et al. Efficacy and safety of recombinant human adenovirus type 5 (H101) in persistent, recurrent, or metastatic gynecologic malignancies: a retrospective study[J]. Front Oncol, 2022, 12: 877155.
doi: 10.3389/fonc.2022.877155 |
| [60] |
ZHANG J, LIU Z, ZHANG Q Y, et al. Successful treatment of a 19-year-old patient with locally advanced clear cell adenocarcinoma of the uterine cervix using recombinant human adenovirus type 5 (Oncorine) combined with chemoradiotherapy: a case report[J]. Ann Transl Med, 2021, 9(23): 1747.
doi: 10.21037/atm-21-5963 pmid: 35071441 |
| [61] |
HSU K F, WU C L, HUANG S C, et al. Conditionally replicating E1B-deleted adenovirus driven by the squamous cell carcinoma antigen 2 promoter for uterine cervical cancer therapy[J]. Cancer Gene Ther, 2008, 15(8): 526-534.
doi: 10.1038/cgt.2008.37 pmid: 18497852 |
| [62] |
DUAN Y X, BAI H X, LI X, et al. Oncolytic adenovirus H101 synergizes with radiation in cervical cancer cells[J]. Curr Cancer Drug Targets, 2021, 21(7): 619-630.
doi: 10.2174/1568009621666210308103541 |
| [63] |
KAGABU M, YOSHINO N, SAITO T, et al. The efficacy of a third-generation oncolytic herpes simplex viral therapy for an HPV-related uterine cervical cancer model[J]. Int J Clin Oncol, 2021, 26(3): 591-597.
doi: 10.1007/s10147-020-01823-6 pmid: 33146805 |
| [64] |
PACKIAM V T, LAMM D L, BAROCAS D A, et al. An open label, single-arm, phase Ⅱ multicenter study of the safety and efficacy of CG0070 oncolytic vector regimen in patients with BCG-unresponsive non-muscle-invasive bladder cancer: interim results[J]. Urol Oncol, 2018, 36(10): 440-447.
doi: 10.1016/j.urolonc.2017.07.005 |
| [65] |
BURKE J M, LAMM D L, MENG M V, et al. A first in human phase 1 study of CG0070, a GM-CSF expressing oncolytic adenovirus, for the treatment of nonmuscle invasive bladder cancer[J]. J Urol, 2012, 188(6): 2391-2397.
doi: 10.1016/j.juro.2012.07.097 pmid: 23088985 |
| [66] |
ZHANG R, CUI Y X, GUAN X, et al. A recombinant human adenovirus type 5 (H101) combined with chemotherapy for advanced gastric carcinoma: a retrospective cohort study[J]. Front Oncol, 2021, 11: 752504.
doi: 10.3389/fonc.2021.752504 |
| [67] | 徐瑞华, 袁中玉, 管忠震, 等. 瘤内注射E1B缺失腺病毒治疗恶性肿瘤的Ⅱ期临床研究[J]. 中国癌症杂志, 2004, 14(1): 12-14. |
| XU R H, YUAN Z Y, GUAN Z Z, et al. Phase Ⅱ clinical study of intratumoral H101, an E1B deleted adenovirus, in patients with cancer[J]. China Oncol, 2004, 14(1): 12-14. | |
| [68] | 李永强, 胡晓桦, 谢伟敏, 等.p14ARF、 p53蛋白表达与H101治疗鼻咽癌疗效的关系[J]. 肿瘤, 2007, 27(5): 390-392. |
| LI Y Q, HU X H, XIE W M, et al. Relationship between the expressions of p14ARF and p53 proteins and the therapeutic efficacy of H101 on nasopharyngeal carcinoma[J]. Tumor, 2007, 27(5): 390-392. | |
| [69] |
ROGULSKI K R, FREYTAG S O, ZHANG K, et al. In vivo antitumor activity of ONYX-015 is influenced by p53 status and is augmented by radiotherapy[J]. Cancer Res, 2000, 60(5): 1193-1196.
pmid: 10728673 |
| [70] | NEMUNAITIS J, GANLY I, KHURI F, et al. Selective replication and oncolysis in p53 mutant tumors with ONYX-015, an E1B-55kD gene-deleted adenovirus, in patients with advanced head and neck cancer: a phase Ⅱ trial[J]. Cancer Res, 2000, 60(22): 6359-6366. |
| [71] |
MCCORMICK F. Interactions between adenovirus proteins and the p53 pathway: the development of ONYX-015[J]. Semin Cancer Biol, 2000, 10(6): 453-459.
pmid: 11170867 |
| [72] |
HEISE C, SAMPSON-JOHANNES A, WILLIAMS A, et al. ONYX-015, an E1B gene-attenuated adenovirus, causes tumor-specific cytolysis and antitumoral efficacy that can be augmented by standard chemotherapeutic agents[J]. Nat Med, 1997, 3(6): 639-645.
pmid: 9176490 |
| [73] |
GEOERGER B, GRILL J, OPOLON P, et al. Oncolytic activity of the E1B-55 kDa-deleted adenovirus ONYX-015 is independent of cellular p53 status in human malignant glioma xenografts[J]. Cancer Res, 2002, 62(3): 764-772.
pmid: 11830531 |
| [74] |
O’SHEA C C, JOHNSON L, BAGUS B, et al. Late viral RNA export, rather than p53 inactivation, determines ONYX-015 tumor selectivity[J]. Cancer Cell, 2004, 6(6): 611-623.
doi: 10.1016/j.ccr.2004.11.012 pmid: 15607965 |
| [75] | 李永强, 胡晓桦, 谢伟敏, 等. p53基因表达与H101治疗恶性肿瘤疗效的关系[J]. 广西医科大学学报, 2006, 23(6): 951-952. |
| LI Y Q, HU X H, XIE W M, et al. Relationship between p53 gene expression and therapeutic effect of H101 on malignant tumor[J]. J Guangxi Med Univ, 2006, 23(6): 951-952. | |
| [76] |
WANG C J, XIAO C W, YOU T G, et al. Interferon-α enhances antitumor activities of oncolytic adenovirus-mediated IL-24 expression in hepatocellular carcinoma[J]. Mol Cancer, 2012, 11: 31.
doi: 10.1186/1476-4598-11-31 |
| [77] |
YING L, CHENG H, XIONG X W, et al. Interferon alpha antagonizes the anti-hepatoma activity of the oncolytic virus M1 by stimulating anti-viral immunity[J]. Oncotarget, 2017, 8(15): 24694-24705.
doi: 10.18632/oncotarget.15788 pmid: 28445966 |
| [78] |
HAINES B B, DENSLOW A, GRZESIK P, et al. ONCR-177, an oncolytic HSV-1 designed to potently activate systemic antitumor immunity[J]. Cancer Immunol Res, 2021, 9(3): 291-308.
doi: 10.1158/2326-6066.CIR-20-0609 pmid: 33355229 |
| [79] |
BREITBACH C J, BURKE J, JONKER D, et al. Intravenous delivery of a multi-mechanistic cancer-targeted oncolytic poxvirus in humans[J]. Nature, 2011, 477(7362): 99-102.
doi: 10.1038/nature10358 |
| [80] |
FREEMAN A I, ZAKAY-RONES Z, GOMORI J M, et al. Phase Ⅰ/Ⅱ trial of intravenous NDV-HUJ oncolytic virus in recurrent glioblastoma multiforme[J]. Mol Ther, 2006, 13(1): 221-228.
doi: 10.1016/j.ymthe.2005.08.016 |
| [81] |
NEMUNAITIS J, CUNNINGHAM C, BUCHANAN A, et al. Intravenous infusion of a replication-selective adenovirus (ONYX-015) in cancer patients: safety, feasibility and biological activity[J]. Gene Ther, 2001, 8(10): 746-759.
doi: 10.1038/sj.gt.3301424 pmid: 11420638 |
| [82] |
SHEN A, LIU S H, YU W Q, et al. p53 gene therapy-based transarterial chemoembolization for unresectable hepatocellular carcinoma: a prospective cohort study[J]. J Gastroenterol Hepatol, 2015, 30(11): 1651-1656.
doi: 10.1111/jgh.13009 |
| [83] | REID T, GALANIS E, ABBRUZZESE J, et al. Hepatic arterial infusion of a replication-selective oncolytic adenovirus (dl1520): phase Ⅱ viral, immunologic, and clinical endpoints[J]. Cancer Res, 2002, 62(21): 6070-6079. |
| [84] |
DE GRAAF J F, HUBERTS M, FOUCHIER R A M, et al. Determinants of the efficacy of viro-immunotherapy: a review[J]. Cytokine Growth Factor Rev, 2020, 56: 124-132.
doi: 10.1016/j.cytogfr.2020.07.001 |
| [85] |
HARRINGTON K, FREEMAN D J, KELLY B, et al. Optimizing oncolytic virotherapy in cancer treatment[J]. Nat Rev Drug Discov, 2019, 18(9): 689-706.
doi: 10.1038/s41573-019-0029-0 pmid: 31292532 |
| [86] |
BOMMAREDDY P K, SHETTIGAR M, KAUFMAN H L. Integrating oncolytic viruses in combination cancer immunotherapy[J]. Nat Rev Immunol, 2018, 18(8): 498-513.
doi: 10.1038/s41577-018-0014-6 pmid: 29743717 |
| [87] |
TIAN G, LIU J L, ZHOU J S, et al. Multiple hepatic arterial injections of recombinant adenovirus p53 and 5-fluorouracil after transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: a pilot phase Ⅱ trial[J]. Anticancer Drugs, 2009, 20(5): 389-395.
doi: 10.1097/CAD.0b013e32832a2df9 |
| [88] | 袁中玉, 张力, 李苏, 等. E1B缺失腺病毒瘤内注射治疗恶性肿瘤的安全性研究[J]. 癌症, 2003, 22(3): 310-313. |
| YUAN Z Y, ZHANG L, LI S, et al. Safety of an E1B deleted adenovirus administered intratumorally to patients with cancer[J]. Chin J Cancer, 2003, 22(3): 310-313. | |
| [89] | 徐瑞华, 袁中玉, 管忠震, 等. 瘤内注射E1B缺失腺病毒(H101)与化疗联合治疗恶性肿瘤的Ⅱ期临床试验[J]. 癌症, 2003, 22(12): 1307-1310. |
| XU R H, YUAN Z Y, GUAN Z Z, et al. Phase Ⅱ clinical study of intratumoral H101, an E1B deleted adenovirus, in comb ination with chemotherapy in patients with cancer[J]. Chin J Cancer, 2003, 22(12): 1307-1310. | |
| [90] |
GORADEL N H, BAKER A T, ARASHKIA A, et al. Oncolytic virotherapy: challenges and solutions[J]. Curr Probl Cancer, 2021, 45(1): 100639.
doi: 10.1016/j.currproblcancer.2020.100639 |
| [1] | XU Rui, WANG Zehao, WU Jiong. Advances in the role of tumor-associated neutrophils in the development of breast cancer [J]. China Oncology, 2024, 34(9): 881-889. |
| [2] | Committee of Integrated Rehabilitation for Urogenital Tumors, Chinese Anti-Cancer Association. Chinese expert consensus on perioperative integrated rehabilitation for radical prostatectomy (2024 edition) [J]. China Oncology, 2024, 34(9): 890-902. |
| [3] | XIAO Yi, WU Ming, YAO Gang. Research progress and future perspectives of tumor organoid [J]. China Oncology, 2024, 34(8): 763-776. |
| [4] | CAO Xiaoshan, YANG Beibei, CONG Binbin, LIU Hong. The progress of treatment for brain metastases of triple-negative breast cancer [J]. China Oncology, 2024, 34(8): 777-784. |
| [5] | LIU Shuai, ZHANG Kai, ZHANG Xiaoqing, LUAN Wei. An exploratory study on the perioperative treatment of locally advanced gastric cancer with combination of penpulimab, anlotinib and chemotherapy [J]. China Oncology, 2024, 34(7): 659-668. |
| [6] | LIAO Ziyi, PENG Yang, ZENG Beilei, MA Yingying, ZENG Li, GAN Kelun, MA Daiyuan. Analysis of pathological remission degree and influencing factors of radical surgery after neoadjuvant immunotherapy combined with chemotherapy in patients with locally advanced esophageal squamous cell carcinoma [J]. China Oncology, 2024, 34(7): 669-679. |
| [7] | LIANG Yingyun, CHEN Jianhua. Application progress of oncolytic virus combined with immunotherapy in the treatment of malignant tumors [J]. China Oncology, 2024, 34(7): 686-694. |
| [8] | HUANG Sijie, KANG Xun, LI Wenbin. Clinical research progress of intrathecal therapy in the treatment of leptomeningeal metastasis [J]. China Oncology, 2024, 34(7): 695-701. |
| [9] | Cancer Nuclear Medicine Committee of China Anti-Cancer Association, Chinese Association of Nuclear Medicine Physicians. Expert consensus of 177Lu-labeled PSMA radioligand therapy for clinical practice of prostate cancer (2024 edition) [J]. China Oncology, 2024, 34(7): 702-714. |
| [10] | TANG Nan, HUANG Huixia, LIU Xiaojian. Integrated single-cell sequencing and transcriptome sequencing to reveal a 9-gene prognostic signature of immune cells in colorectal cancer [J]. China Oncology, 2024, 34(6): 548-560. |
| [11] | XIN Meiyi, LIN Yuhong, ZHAO Kai. Progress in the development of mRNA vaccine and its delivery systems for anti-tumor immunotherapy [J]. China Oncology, 2024, 34(5): 509-516. |
| [12] | Professional Committee on Gastric Cancer of Shanghai Anticancer Association , Professional Committee on Gastrointestinal Cancer of China Association for Promotion of Health Science and Technology . Chinese expert consensus on clinical practice of locally advanced gastric cancer invading adjacent organs (2024 edition) [J]. China Oncology, 2024, 34(5): 517-526. |
| [13] | XU Yuchen, ZHANG Jian, WANG Yan, LIN Jinyi, ZHOU Yuhong, CHENG Leilei, GE Junbo. Therapeutic effects of tofacitinib on steroid-resistant immune checkpoint inhibitor-associated myocarditis [J]. China Oncology, 2024, 34(4): 400-408. |
| [14] | XU Yonghu, XU Dazhi. Progress and prospects of gastric cancer treatment in the 21st century [J]. China Oncology, 2024, 34(3): 239-249. |
| [15] | XUE Chi, GAO Peng, ZHU Zhi, WANG Zhenning. Application and challenge of immunotherapy in perioperative therapy of gastric cancer [J]. China Oncology, 2024, 34(3): 259-267. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd