Welcome to China Oncology,
China Oncology ›› 2023, Vol. 33 ›› Issue (6): 597-604.doi: 10.19401/j.cnki.1007-3639.2023.06.007
• Article • Previous Articles Next Articles
DU Shuxiang1( ), ZHAO Yingzhi1, ZHANG Xuetao1, WANG Tao1, LUO Jingyu2, ZHANG Wei1, WU Gang1()
), ZHAO Yingzhi1, ZHANG Xuetao1, WANG Tao1, LUO Jingyu2, ZHANG Wei1, WU Gang1()
Received:2022-08-10
Revised:2023-03-14
Online:2023-06-30
Published:2023-07-26
Share article
CLC Number:
DU Shuxiang, ZHAO Yingzhi, ZHANG Xuetao, WANG Tao, LUO Jingyu, ZHANG Wei, WU Gang. Analysis of group 12a lymph node metastasis at different sites of gastric adenocarcinoma and its risk factors[J]. China Oncology, 2023, 33(6): 597-604.
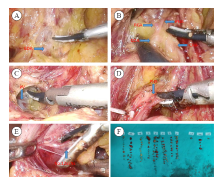
Fig. 1
Lymph node dissection steps in group No.12a GDA: The gastroduodenal artery; RGA: The right gastric artery; CHA: The common hepatic artery; PHA: The proper hepatic artery; PV: The portal vein. A: Severed the right gastroomentum artery, free the gastroduodenal artery; B: Bared the common hepatic artery, the right gastric artery and the proper hepatic artery; C: Exposed the portal vein, separate along the front of the portal vein, and clean the lymph nodes between the portal vein and the liver intrinsic artery; D: Lifted down the intrinsic artery of the liver to sweep away the surrounding adipose tissue; E: Opened the hepatoduodenal ligament and clean the 12a group lymph nodes; F: Lymph nodes were picked in groups within 30minutes after the specimen is left."
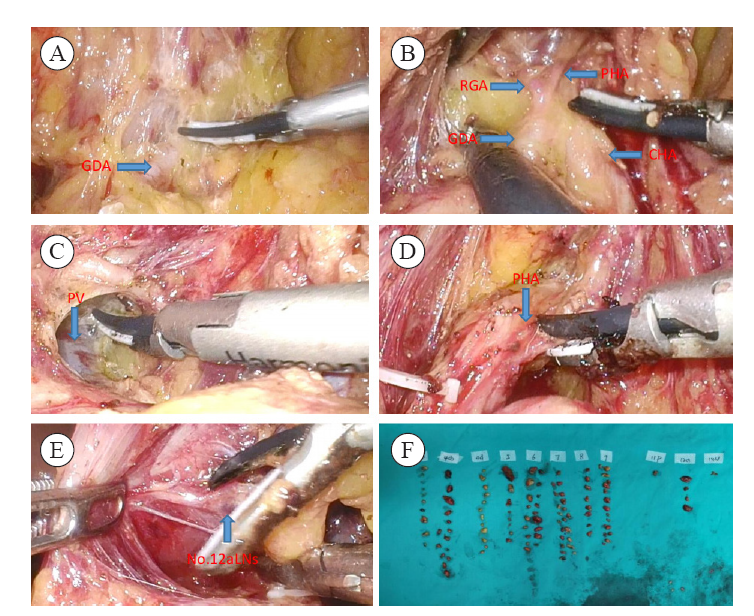
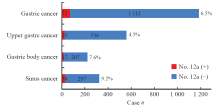
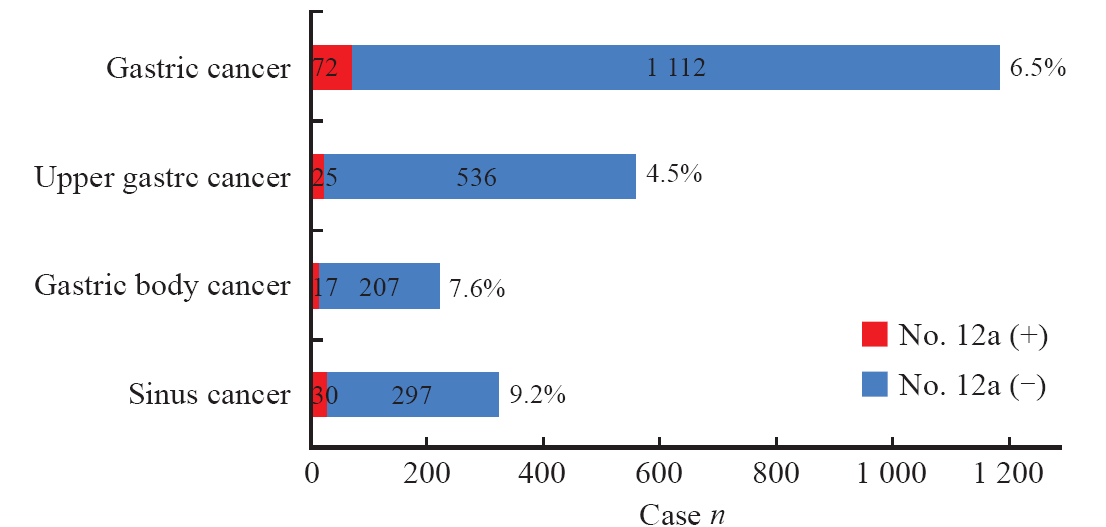
Fig. 2
Lymph node metastasis rate of the group 12a lymph node in each location"
Tab. 1
The subgroup analysis and univariate analysis of No.12a lymph node metastasis in gastric cancer in each location [n (%)]"
| Clinicopathological data | Upper cancer (n=561) | Body cancer (n=224) | Antral cancer (n=327) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No.12a (+) (n=25) | No.12a (-) (n=536) | χ2 | P value | No.12a (+) (n=17) | No.12a (-) (n=207) | χ2 | P value | No.12a (+) (n=30) | No.12a (-) (n=297) | χ2 | P value | |||
| Gender | 0.841 | 0.359 | 0.829 | 0.362 | 0.984 | 0.321 | ||||||||
| Male | 16 (5.2) | 293 (94.8) | 7 (9.3) | 109 (90.7) | 19 (10.6) | 160 (89.4) | ||||||||
| Female | 9 (3.6) | 243 (96.4) | 10 (9.2) | 98 (90.8) | 11 (7.4) | 137 (92.6) | ||||||||
| Age/year | 0.066 | 0.789 | 0.200 | 0.654 | 0.066 | 0.767 | ||||||||
| <65 | 14 (4.3) | 314 (95.7) | 10 (7.0) | 133 (93.0) | 13 (8.7) | 136 (91.3) | ||||||||
| ≥65 | 11 (4.7) | 222 (95.3) | 7 (8.6) | 74 (91.4) | 17 (9.6) | 161 (90.4) | ||||||||
| BMI/(kg·m-2) | 5.562 | 0.018 | 3.100 | 0.078 | 14.064 | <0.001 | ||||||||
| <24 | 14 (3.3) | 411 (96.7) | 16 (9.3) | 156 (90.7) | 13 (5.8) | 224 (94.2) | ||||||||
| ≥24 | 11 (8.1) | 125 (91.9) | 1 (1.9) | 51 (98.2) | 17 (18.9) | 73 (81.1) | ||||||||
| Tumor size D/cm | 155.058 | <0.001 | 90.044 | <0.001 | 137.080 | <0.001 | ||||||||
| <6 | 0 (0.0) | 480 (100.0) | 0 (0.0) | 186 (100.0) | 6 (2.1) | 280 (97.9) | ||||||||
| ≥6 | 25 (30.9) | 56 (69.1) | 17 (44.7) | 21 (55.3) | 24 (58.5) | 17 (41.5) | ||||||||
| Borrmann‘s classification | 1.351 | 0.509 | 0.112 | 0.946 | 4.999 | 0.082 | ||||||||
| Uplift | 2 (4.9) | 39 (95.1) | 1 (8.3) | 11 (91.7) | 1 (5.6) | 17 (94.4) | ||||||||
| Ulcer | 20 (4.1) | 466 (95.9) | 15 (9.3) | 150 (90.7) | 25 (8.4) | 273 (91.6) | ||||||||
| Infiltrating | 3 (8.8) | 31(91.2) | 1 (6.7) | 14 (93.3) | 4 (9.3) | 7 (90.7) | ||||||||
| Differentiation | 0.325 | 0.569 | 0.888 | 0.346 | 3.545 | 0.060 | ||||||||
| Poorly differentiated | 4 (3.5) | 111(96.5) | 5 (10.9) | 41 (89.1) | 10 (15.2) | 56 (84.8) | ||||||||
| Medium to high differentiation | 21 (4.7) | 425 (95.3) | 12(6.7) | 166(93.3) | 20 (7.7) | 241 (92.3) | ||||||||
| pT staging | 0.454 | 0.011 | 8.362 | 0.004 | 13.167 | <0.001 | ||||||||
| T1-T2 | 0 (0.0) | 111 (100.0) | 0 (0.0) | 70 (100.0) | 1 (9.3) | 107 (90.7) | ||||||||
| T3-T4 | 25(5.6) | 425 (94.4) | 17(11.0) | 137 (99.0) | 29 (13.2) | 190 (86.8) | ||||||||
| pN staging | 39.075 | <0.001 | 4.303 | 0.038 | 88.328 | <0.001 | ||||||||
| N0-N1 | 0 (0.0) | 336 (100.0) | 0 (0.0) | 123 (100.0) | 0 (0.0) | 238 (100.0) | ||||||||
| N2-N3 | 25 (11.1) | 200 (88.9) | 3 (3.4) | 84 (96.6) | 30 (33.7) | 59 (66.3) | ||||||||
| TNM staging | 20.251 | <0.001 | 9.330 | 0.002 | 7.882 | 0.005 | ||||||||
| Ⅰ-Ⅱ | 1 (0.4) | 268 (99.6) | 2 (1.9) | 104 (98.1) | 0 (0.0) | 63 (100.0) | ||||||||
| Ⅲ-Ⅳ | 24 (8.2) | 268 (91.8) | 15 (12.7) | 103 (87.3) | 30 (11.4) | 234 (88.6) | ||||||||
| Neurovascular invasion | 0.067 | 0.769 | 10.695 | 0.001 | 2.384 | 0.123 | ||||||||
| Yes | 14 (4.7) | 286 (95.3) | 8 (20.0) | 32 (80.0) | 14 (12.6) | 97 (87.4) | ||||||||
| No | 11 (4.2) | 250 (95.8) | 9 (4.9) | 175 (95.1) | 16 (7.4) | 200 (92.6) | ||||||||
Tab. 2
Variable assignment table"
| Variable | Assignment table |
|---|---|
| Dependent variable | No.12a lymph node metastasis was 1; Lymph node metastasis in No.12a was 0 |
| Independent variable | |
| BMI | ≥24 kg/m2 was“1”, <24 kg/m² was “0” |
| Tumor size | ≥6 cm was “1”, <6 cm was “0” |
| pT staging | T1 was “1”, T2 was “2”, T3 was “3”, T4 was “4” |
| TNM staging | Ⅰ was “1”, Ⅱ was “2”, Ⅲ was “3” |
| Vascular nerve invasion | “Yes” was “1”,“No”was“0” |
Tab. 3
Multivariable logistic regression analysis of risk factors for No.12a lymph node metastasis in upper gastric cancer"
| Variable | β | SE | Wald χ2 | P value | OR | 95% CI |
|---|---|---|---|---|---|---|
| BMI | -0.050 | 0.030 | 2.844 | 0.092 | 0.951 | 0.898-1.008 |
| Tumor size | 1.139 | 0.038 | 877.688 | <0.001 | 3.122 | 2.896-3.366 |
| pT staging | 0.878 | 0.176 | 24.982 | <0.001 | 2.406 | 1.705-3.396 |
| TNM staging | 2.068 | 0.260 | 63.415 | <0.001 | 7.910 | 4.755-13.160 |
Tab. 4
Multivariable logistic regression analysis of risk factors for No.12a lymph node metastasis in gastric antral cancer"
| Variable | β | SE | Wald χ2 | P value | OR | 95% CI |
|---|---|---|---|---|---|---|
| Tumor size | 1.014 | 0.051 | 394.733 | <0.001 | 2.757 | 2.495-3.047 |
| pT staging | 1.193 | 0.174 | 47.112 | <0.001 | 3.298 | 2.346-4.638 |
| TNM staging | 0.164 | 0.189 | 0.747 | 0.388 | 1.178 | 0.813-1.707 |
| Vascular nerve invasion | 0.609 | 0.151 | 16.275 | <0.001 | 1.839 | 1.368-2.473 |
Tab. 5
Multivariable logistic regression analysis of risk factors for No.12a lymph node metastasis in gastric body cancer group"
| Variable | β | SE | Wald χ2 | P value | OR | 95% CI |
|---|---|---|---|---|---|---|
| BMI | 0.093 | 0.036 | 6.691 | 0.01 | 1.098 | 1.023-1.178 |
| Tumor size | 1.053 | 0.243 | 18.708 | <0.001 | 2.865 | 1.778-4.616 |
| pT staging | 2.602 | 0.244 | 113.565 | <0.001 | 13.497 | 8.363-21.783 |
| TNM staging | 1.337 | 0.103 | 169.942 | <0.001 | 3.806 | 3.113-4.653 |
| [1] |
SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249.
doi: 10.3322/caac.v71.3 |
| [2] | 李国新. 胃癌外科2021年研究进展及学科展望[J]. 中华胃肠外科杂志, 2022, 25(1): 15-21. |
| LI G X. Research progress and prospect of gastric cancer surgery in 2021[J]. Chin J Gastrointest Surg, 2022, 25(1): 15-21. | |
| [3] |
DONG Y P, CAI F L, WU Z Z, et al. Risk of station 12a lymph node metastasis in patients with lower-third gastric cancer[J]. World J Gastrointest Surg, 2021, 13(11): 1390-1404.
doi: 10.4240/wjgs.v13.i11.1390 |
| [4] |
SIERRA A, REGUEIRA F M, HERNÁNDEZ-LIZOÁIN J L, et al. Role of the extended lymphadenectomy in gastric cancer surgery: experience in a single institution[J]. Ann Surg Oncol, 2003, 10(3): 219-226.
pmid: 12679305 |
| [5] |
JAPANESE GASTRIC CANCER ASSOCIATION. Japanese gastric cancer treatment guidelines 2018 (5th edition)[J]. Gastric Cancer, 2021, 24(1): 1-21.
doi: 10.1007/s10120-020-01042-y |
| [6] |
JAPANESE GASTRIC CANCER ASSOCIATION. Japanese classification of gastric carcinoma-2nd English edition[J]. Gastric Cancer, 1998, 1(1): 10-24.
doi: 10.1007/PL00011681 |
| [7] |
EDGE S B, COMPTON C C. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM[J]. Ann Surg Oncol, 2010, 17(6): 1471-1474.
doi: 10.1245/s10434-010-0985-4 pmid: 20180029 |
| [8] |
LU J, ZHENG C H, CAO L L, et al. The effectiveness of the 8th American Joint Committee on Cancer TNM classification in the prognosis evaluation of gastric cancer patients: a comparative study between the 7th and 8th editions[J]. Eur J Surg Oncol, 2017, 43(12): 2349-2356.
doi: S0748-7983(17)30659-5 pmid: 28943179 |
| [9] |
HARTGRINK H H, VAN DE VELDE C J, PUTTER H, et al. Extended lymph node dissection for gastric cancer: who may benefit? Final results of the randomized Dutch gastric cancer group trial[J]. J Clin Oncol, 2004, 22(11): 2069-2077.
doi: 10.1200/JCO.2004.08.026 pmid: 15082726 |
| [10] |
CUSCHIERI A, WEEDEN S, FIELDING J, et al. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Surgical Co-operative Group[J]. Br J Cancer, 1999, 79(9/10): 1522-1530.
doi: 10.1038/sj.bjc.6690243 |
| [11] |
KONG S H, YOO M W, KIM J W, et al. Validation of limited lymphadenectomy for lower-third gastric cancer based on depth of tumour invasion[J]. Br J Surg, 2011, 98(1): 65-72.
doi: 10.1002/bjs.7266 pmid: 20954197 |
| [12] | WEI Z W, XIA G K, WU Y, et al. Evaluation of skeletonization of the hepatoduodenal ligament for the lower third gastric cancer by propensity score analysis[J]. Hepatogastroenterology, 2013, 60(127): 1789-1796. |
| [13] |
CAI S R, CHEN J H, CHEN C Q, et al. Survival of proper hepatic artery lymph node metastasis in patients with gastric cancer: implications for D2 lymphadenectomy[J]. PLoS One, 2015, 10(3): e0118953.
doi: 10.1371/journal.pone.0118953 |
| [14] |
KUMAGAI K, HIKI N, NUNOBE S, et al. Metastasis to the lymph nodes along the proper hepatic artery from adenocarcinoma of the stomach[J]. Langenbecks Arch Surg, 2016, 401(5): 677-685.
doi: 10.1007/s00423-016-1429-9 |
| [15] |
IN H, SOLSKY I, PALIS B, et al. Validation of the 8th edition of the AJCC TNM staging system for gastric cancer using the national cancer database[J]. Ann Surg Oncol, 2017, 24(12): 3683-3691.
doi: 10.1245/s10434-017-6078-x pmid: 28895113 |
| [16] |
CHEN Z H, LIU Y, DOU L Z, et al. The efficacy of the application of the curative criteria of the 5th edition Japanese gastric cancer treatment guidelines for early adenocarcinoma of the esophagogastric junction treated by endoscopic submucosal dissection[J]. Saudi J Gastroenterol, 2021, 27(2): 97-104.
doi: 10.4103/sjg.SJG_403_20 |
| [17] |
AJANI J A, D’AMICO T A, BENTREM D J, et al. Gastric cancer, version 2.2022, NCCN clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2022, 20(2): 167-192.
doi: 10.6004/jnccn.2022.0008 |
| [18] |
SMITH D D, SCHWARZ R R, SCHWARZ R E. Impact of total lymph node count on staging and survival after gastrectomy for gastric cancer: data from a large US-population database[J]. J Clin Oncol, 2005, 23(28): 7114-7124.
doi: 10.1200/JCO.2005.14.621 pmid: 16192595 |
| [19] |
SCHWARZ R E, SMITH D D. Clinical impact of lymphadenectomy extent in resectable gastric cancer of advanced stage[J]. Ann Surg Oncol, 2007, 14(2): 317-328.
doi: 10.1245/s10434-006-9218-2 pmid: 17094022 |
| [20] | SEEVARATNAM R, BOCICARIU A, CARDOSO R, et al. How many lymph nodes should be assessed in patients with gastric cancer? A systematic review[J]. Gastric Cancer, 2012, 15(Suppl 1): S70-S88. |
| [21] | 张晋杰, 王杰, 胡文庆. 进展期胃上部癌淋巴结清扫的现状与研究进展[J]. 中华胃肠外科杂志, 2018, 21(2): 236-240. |
| ZHANG J J, WANG J, HU W Q. Current status and research progress of lymph node dissection in advanced upper gastric cancer[J]. Chin J Gastrointest Surg, 2018, 21(2): 236-240. | |
| [22] | 郑民华, 臧潞, 马君俊, 等. SiewertⅡ型食管胃结合部腺癌腔镜手术治疗中国专家共识(2019版)[J]. 中国实用外科杂志, 2019, 39(11): 1129-1135. |
| ZHENG M H, ZANG L, MA J J, et al. Endoscopic surgery for SiewertⅡ esophagogastric junction adenocarcinoma in China (2019 edition)[J]. Chin J Pract Surg, 2019, 39(11): 1129-1135. | |
| [23] |
SHU P, SUN X F, LIU F L, et al. Pattern of No. 12a lymph node metastasis in gastric cancer[J]. Chin J Cancer Res, 2021, 33(1): 61-68.
doi: 10.21147/j.issn.1000-9604.2021.01.07 |
| [24] |
SATO Y, KATAI H, ITO M, et al. Can proximal gastrectomy be justified for advanced adenocarcinoma of the esophagogastric junction?[J]. J Gastric Cancer, 2018, 18(4): 339-347.
doi: 10.5230/jgc.2018.18.e33 pmid: 30607297 |
| [25] |
WU G, ZHANG D Y, DUAN Y H, et al. Correlations of hemoglobin level and perioperative blood transfusion with the prognosis of gastric cancer: a retrospective study[J]. Med Sci Monit, 2017, 23: 2470-2478.
doi: 10.12659/MSM.900907 |
| [26] |
MITA K, ITO H, KATSUBE T, et al. Prognostic factors affecting survival after multivisceral resection in patients with clinical T4b gastric cancer[J]. J Gastrointest Surg, 2017, 21(12): 1993-1999.
doi: 10.1007/s11605-017-3559-y |
| [27] |
YAMASHITA H, KATAI H, MORITA S, et al. Optimal extent of lymph node dissection for Siewert type Ⅱ esophagogastric junction carcinoma[J]. Ann Surg, 2011, 254(2): 274-280.
doi: 10.1097/SLA.0b013e3182263911 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd