Welcome to China Oncology,
China Oncology ›› 2023, Vol. 33 ›› Issue (12): 1092-1187.doi: 10.19401/j.cnki.1007-3639.2023.12.004
• Guideline and Concensus • Previous Articles Next Articles
The Society of Breast Cancer China Anti-Cancer Association, Breast Oncology Group of the Oncology Branch of the Chinese Medical Association
Received:2023-11-15
Revised:2023-11-30
Online:2023-12-30
Published:2023-12-28
Contact:
SHAO Zhimin.
Share article
CLC Number:
The Society of Breast Cancer China Anti-Cancer Association, Breast Oncology Group of the Oncology Branch of the Chinese Medical Association. Guidelines for breast cancer diagnosis and treatment by China Anti-cancer Association (2024 edition)[J]. China Oncology, 2023, 33(12): 1092-1187.
"
"
"
| 适应证 | 禁忌证 | 豁免前哨淋巴结活检 |
|---|---|---|
| 早期浸润性乳腺癌 | 炎性乳腺癌 | 肿瘤完整切除并经石蜡包埋组织病理完全评估为DCIS |
| 性别不限 | 临床ALN阳性(cN+)并经穿刺活检证实 | ≥70岁(伴随疾病),cT1N0M0,HR阳性HER2阴性,辅助治疗不受腋窝状态影响g |
| 临床ALN阴性(cN0) a | cN+新辅助治疗后仍为阳性 | cT1N0且影像±穿刺活检评估腋淋巴结阴性、接受保乳手术及全乳照射h |
| 单灶或多中心性病变 | cN2-3新辅助治疗后临床阴性 | |
| DCIS全乳切除手术或保乳手术原发肿瘤切除影响随后SLNB成功率和准确性b | ||
| cN0新辅助治疗后临床腋窝阴性 | ||
| 穿刺证实的cN1新辅助治疗后临床腋窝阴性c | ||
| 妊娠患者d | ||
| 保乳联合SLNB术后同侧乳房复发/再发e | ||
| 腋窝淋巴结临床查体阴性但影像学1 ~ 2枚异常并穿刺活检证实转移(有争议的适应证)f |
"
| 危险度a | 判别要点 | |
|---|---|---|
| 区域淋巴结转移 | 其他情况 | |
| 低危 | 阴性 | 同时具备以下条件b:pT≤2 cm;组织学Ⅰ级; LVI阴性; HER2阴性;年龄>35岁; ER/PR阳性c; Ki-67增殖指数≤20%或实验室中位值 |
| ER阳性HER2阴性时, 不满足上述其他条件但多基因检测低危 | ||
| 中危 | 不符合低/高危定义的其他情况 | |
| 高危 | 1 ~ 3枚阳性 | ER/PR阳性且HER2阴性时, 满足以下条件之一d:组织学III级; pT>5 cm;多基因检测高危 |
| ER阴性且PR阴性;或HER2阳性 | ||
| ≥4枚阳性 | 任何情况 | |
"
| 内在分子分型 | 基于IHC4的分子分型 | 备注 |
|---|---|---|
| Luminal A型 | Luminal A样 ER/PR阳性且PR高表达HER2阴性 Ki-67增殖指数低 | ER、PR表达及Ki-67增殖指数的判定值建议采用报告阳性细胞的百分比。 Ki-67增殖指数的判定值在不同病理实验中心可能不同,可采用20%~30%作为判断Ki-67增殖指数高低的界值;同时,以20%作为PR表达高低的判定界值*,可进一步区分Luminal A样和Luminal B样(HER2阴性) |
| Luminal B型 | Luminal B样(HER2阴性) ER/PR阳性 HER2阴性 且Ki-67增殖指数高或PR低表达 | 上述不满足Luminal A样条件的Luminal样肿瘤均可作为Luminal B样亚型 |
| Luminal B样(HER2阳性) ER/PR阳性 HER2阳性(蛋白过表达或基因扩增) 任何状态的Ki-67增殖指数 | ||
| ERBB2+型 | HER2阳性 HER2阳性(蛋白过表达或基因扩增) ER阴性和PR阴性 | |
| Basal-like型 | 三阴性(非特殊型浸润性导管癌) ER阴性 PR阴性HER2阴性 | TNBC和Basal-like型乳腺癌之间的吻合度约80%;但是TNBC也 包含一些特殊类型乳腺癌如分泌性癌和腺样囊性癌等 |
"
| 复发风险度 | 激素受体阳性HER2阴性 | HER2阳性 | TNBC |
|---|---|---|---|
| 低危 | 豁免化疗 | 不适用 | 不适用 |
| 中危且pN0b | ·T3及以上推荐化疗 ·T1b-T2:考虑多基因检测工具,目前指导辅助化疗的主要是21基因或70基因检测 - 21基因:年龄>50岁且RS>25 推荐化疗 - 21基因:年龄≤50岁日RS≥16 推荐化疗 - 70基因:临床高风险a且70基因高风险推荐化疗 - 70基因:临床高风险a且年龄≤50岁且70基因低风险考虑化疗 ·T1b~T2:未接受基因检测,具有如下特征之一的可考虑化疗:ER低表达组织学3级,LVI阳性,年龄≤35岁,高Ki-67增殖指数c ·T1a:原则上豁免化疗,除非同时伴有多个风险因素时个体化综合考虑 | ·T1c及以上推荐 ·T1a-b考虑d ·T1mic原则上不考虑,需个体化综合评估,如年龄、LVI、多灶与否等 | ·T1c及以上推荐 ·T1a-b考虑 ·T1mic原则上不考虑,需个体化综合评估,如年龄、LVI、多灶与否等 |
| 中危且pN1 | ·均推荐化疗 ·除非T1-2且接受21基因或70基因检测时,如下结果才考虑豁免化疗: - 21基因: RS≤11的患者e - 70基因:临床高风险a,70基因低风险且年龄>50岁的患者 | 不适用 | 不适用 |
| 高危 | 均推荐化疗 | 均推荐化疗 | 均推荐化疗 |
"
| 风险度分层 | 初始治疗 | 后续强化治疗 | ||||
|---|---|---|---|---|---|---|
| 推荐 | 考虑 | 可选 | 推荐 | 考虑 | 可选 | |
| 中危(pT1aN0) | ·缺乏高级别证据 | ·wP+H | ·TC+H ·其他个体化方案或临床研究(如口服化疗+H,H+内分泌治疗) | ·无 | - | - |
| 中危(pT1bN0) | ·wP+H | ·TC+H | ·TCbH ·EC-T(wP)+H | ·无 | - | - |
| 中危(pT1c及以上,N0) | ·EC-T(wP)+H ·TCB+H | ·TC+H | ·EC-T(wP)+HP ·TCb+HP | ·无 | - | ·奈拉替尼 |
| 高危(任何pN+) | ·EC-T(wP)+HP ·TCb+HP | - | - | - | ·奈拉替尼 | ·其他TKI |
"
| 分期 | 表现 |
|---|---|
| 0期 | 这是指一种潜在或亚临床状态,尽管淋巴运输受损,组织液/成分发生细微变化,主观症状发生变化,但肿胀仍不明显。 |
| 1期 | 表现为蛋白质含量相对较高的液体早期积聚,随着肢体抬高而消退。各种类型的增殖细胞也可能增加。 |
| 2期 | 涉及实体结构的更多变化,仅肢体抬高很少能减少组织肿胀,凹陷明显。在2期后期,由于皮下脂肪过多和纤维化的发展,肢体可能不会凹陷。 |
| 3期 | 包括淋巴静止性象皮病,在该病中可以不出现凹陷,并出现营养性皮肤变化,如棘皮病、皮肤特征和厚度的改变、脂肪和纤维化的进一步沉积以及疣状过度增生 |
"
"
| 策略 | 目标 |
|---|---|
| 认知疗法或基于网络的认知行为疗法 | ·挑战幸存者对睡眠障碍的不适应信念和误解 |
| 刺激控制 | ·床与卧室仅用于睡眠的场所 |
| 睡眠限制 | ·通过以下方式改善睡眠连续性: ·限制卧床时间 ·每天相对固定的就寝和起床时间来保持睡眠节律 |
| 放松训练 | ·减少睡前的生理和认知唤醒 ·技术包括渐进式肌肉放松、深呼吸、冥想、瑜伽和生物反馈 ·可视化 |
"
| 药物名称 | 有助于睡眠启动 | 增加总睡眠时间 | 用于睡眠启动和维持 |
|---|---|---|---|
| 唑吡坦 | + | + | - |
| 扎勒布隆 | + | - | - |
| 右佐匹克隆 | + | + | + |
| 拉米替隆 | + | ± | - |
| 替马西泮 | + | + | + |
| 多塞平(3~6 mg) | + | + | + |
"
| 请回答以下关于你整体性功能的问题: | |
|---|---|
| 你对自己的性功能满意吗?如有,请继续回答下列问题: | |
| 你的性功能问题是; | |
| 1 | 对性几乎没有兴趣; |
| 2 | 生殖器感觉下降; |
| 3 | 阴道润滑减少(干燥); |
| 4 | 无法达到性高潮; |
| 5 | 性生活中的阴道疼痛; |
| 6 | 其他问题: |
| 哪一个问题对您困扰最大,请您圈出序号 1 2 3 4 5 6 | |
| 你想就诊时和你的医生谈谈吗? 是 否 | |
"
"
"
| 专家观点 | 推荐使用 骨改良药物 | 不推荐使用骨改良药物 |
|---|---|---|
| 骨转移引起的高钙血症 | √ | |
| 骨转移引起的骨痛 | √ | |
| ECT异常,X线(或CT、或MRI)证实的骨转移 | √ | |
| ECT异常,X线正常,但CT或MRI显示骨破坏 | √ | |
| 影像学诊断为骨破坏,即使没有骨痛症状 | √ | |
| ECT异常,X线正常,且CT或MRI也未显示骨破坏 | √ | |
| 存在骨转移风险(乳酸脱氢酶升高或碱性磷酸酶升高)的患者 | √ |

"

"

"
"
"
| 推荐对乳腺癌患者进行BRCA基因检测的专家共识 |
|---|
| ·家族中有已知的BRCA1/2基因有害突变 |
| ·乳腺癌病史符合以下条件: |
| 确诊年龄≤45岁 |
| 确诊年龄46 ~ 50岁 |
| ▲第二原发乳腺癌 |
| ▲≥1位直系亲属确诊乳腺癌,其确诊年龄不限 |
| ▲≥1位直系亲属确诊高级别前列腺癌(Gleason分值≥7分) |
| ▲有限或未知家族史 |
| 三阴性乳腺癌确诊年龄≤60岁 |
| 年龄不限,但符合以下一项条件 |
| ▲≥1位直系亲属且满足:乳腺癌确诊年龄≤50岁,或卵巢癌,或男性乳腺癌,或转移性前列腺癌,或胰腺癌 |
| ▲≥2位患者或直系亲属确诊乳腺癌 |
| ·卵巢癌病史 |
| ·男性乳腺癌病史 |
| ·胰腺癌病史 |
| ·转移性前列腺癌病史 |
| ·任何年龄的高级别前列腺癌病史(Gleason分值≥7分)并且符合以下1项条件: |
| ▲≥1位直系亲属确诊卵巢癌、胰腺癌或转移性前列腺癌,确诊年龄不限或乳腺癌确诊年龄≤50岁 |
| ▲≥2位直系亲属确诊乳腺癌、前列腺癌(任何级别),确诊年龄不限 |
| ·肿瘤中发现BRCA1/2有害突变且胚系突变状态未明 |
| ·无论家族史,BRCA突变相关癌症受益于靶向治疗(如卵巢癌/HER2阴性的转移性乳腺癌PARP抑制剂治疗,前列腺癌铂类药物化疗 |
| ·不符合以上标准但有≥1位一级或二级亲属符合以上任何一条的个体。对于未携带者(BRCA1/2有害突变)检测结果的解读是有局限性的,需要充分讨论 |
"
| 患者姓名:××× | 性别:女 | 年龄:51岁 | 放射学检查号码:12345678 |
|---|---|---|---|
| 门诊号: | 住院号:123456 | 科室:乳腺外科 | 病区: |
| 临床诊断:左乳肿块 | |||
| 检查日期:2023年10月10日前片无 | |||
| 投照体位: | |||
| √ 左侧:头足(轴)位、侧斜位 | |||
| 检查设备GE2000D | |||
| √ 右侧:头足(轴)位、侧斜位 | |||
| 影像学描述: | |||
| 双侧乳腺腺体不均匀致密型。 | |||
| 左乳腺外上方可见一大小2.8 cm×1.8 cm的肿块影,高密度,形态不规则并伴有边缘毛刺,内见多形性细小钙化。 | |||
| 右乳腺未见明显肿块与异常钙化。 | |||
| 双侧皮肤、乳头影正常。 | |||
| 双侧腋下可见小淋巴结,形态密度无异常。 | |||
| 影像学评估: | |||
| 左乳外上病灶,考虑为恶性,BI-RADS 5。 | |||
| 右乳未见异常,BI-RADS 1。 | |||
"
| 患者姓名:××× | 年龄: | 性别: | 超声号: |
|---|---|---|---|
| 住院/门诊号: | 临床诊断: | 使用仪器: | 探头频率: |
| 双侧(左侧、右侧)乳腺组织回声(不)均匀,结构清晰(紊乱)。 | |||
| 导管(未见)扩张(内径 mm),乳腺组织呈条索状(结节状、团块状)等回声。 | |||
| 左(右)乳腺外上象限(内上、内下、外下、乳晕区域)点(按时钟法)距乳头 cm,探及低(等、高)回声结节,大小 mm× mm× mm,形态(不)规则,边界(欠、不)清晰,边缘光整(毛刺、成角、分叶状),内部回声(欠、不)均匀,(未)见点状强回声,后方回声增强(无变化、衰减),周围组织(水肿、受压、变形、无变化),彩色多普勒超声显示内部(无)血流信号,呈点状(条状、网状、团状),RI 。 | |||
| 双(左、右)腋下见淋巴结,大小 mm× mm× mm,形态(不)规则,边界(欠、不)清晰,边缘光整(毛刺、成角、分叶状),内部回声(欠、不)均匀,(未)见点状强回声,后方回声增强(无变化、衰减),彩色多普勒超声显示内部(无)血流信号,呈点状(条状、网状、团状),RI 。 | |||
| 超声提示: | |||
| 1. 双(左、右)乳未见明显占位 | |||
| 2. 左(右)乳外上象限实性(混合性、囊性)占位(纤维瘤可能……) | |||
| 检查医师: | |||
| 检查日期: | |||
"
| 患者姓名:××× | 性别:女 | 年龄:51 | 放射学检查号码:12345678 |
|---|---|---|---|
| 门诊号: | 住院号:123456 | 科室:乳腺外科 | 病区: |
| 临床病史:右乳癌待排检 | |||
| 要求:常规动态增强扫描 | |||
| 检查日期: | |||
| 前片:无 | |||
| 检查部位和名称:双侧乳房(平扫+动态增强) | |||
| 检查设备:3 T/1.5 T,乳腺专用线圈 | |||
| 检查方法:平扫AxT1,AxT2;Ax+Sag C+;以速率2.5 mL/s注射轧对比剂(具体药名)15 mL,再用0.9%的生理盐水10 mL冲洗 | |||
| 临床简述: | |||
| 右乳外上扪及肿块,X线和超声检查提示病变性质不确定。末次月经时间: (或绝经后妇女)。 | |||
| 影像学描述: | |||
| 两侧乳房大小、形态基本对称,两侧纤维腺体呈不均质致密型,分布无异常,增强后实质背景轻度强化。右乳外上象限中带见一卵圆形肿块影,边缘模糊不清,T1WI上呈低信号,T2WI上高信号,增强后呈不规则环形强化,早期强化明显,延迟期强化降低,动态增强曲线呈廓清型。病变大小约3 cm×2 cm×2 cm。病灶在扩散加权上受限,ADC约0.9 mm2/s。病灶前缘距离乳头约3 cm。左乳内未见明确占位及异常强化影。所示两侧腋下未见明显肿大淋巴结,两侧胸壁肌肉未见异常。两侧乳头及皮肤未见明显异常。 | |||
| 影像学评估: | |||
| 右乳外上象限中带距离乳头约3 cm处肿块,高度怀疑其为恶性,建议活检,BI-RADS 5 | |||
| 左乳未见异常发现,BI-RADS 1 | |||
| 报告医师签名: | |||
| 审核医师签名: | |||
| 报告日期: | |||
"
| MP分级 | 特征 |
|---|---|
| MP分级(1级) | 浸润癌细胞无改变或仅个别癌细胞发生改变,癌细胞数量总体未减少 |
| MP分级(2级) | 浸润癌细胞轻度减少,但总数量仍高,癌细胞减少不超过30% |
| MP分级(3级) | 浸润癌细胞减少介于30% ~ 90% |
| MP分级(4级) | 浸润癌细胞显著减少超过90%,仅残存散在小簇状癌细胞或单个癌细胞 |
| MP分级(5级) | 原肿瘤瘤床部位已无浸润癌细胞,但可存在导管原位癌 |
"
| 乳腺组织学分型 |
|---|
| 乳头状肿瘤 |
| 乳头状导管原位癌 |
| 包被性乳头状癌 |
| 实性乳头状癌(原位或浸润) |
| 浸润性乳头状癌 |
| 小叶原位癌 |
| 导管原位癌 |
| 浸润性乳腺癌 |
| 浸润性癌,非特殊类型 |
| 微浸润性癌 |
| 浸润性小叶癌 |
| 小管癌 |
| 筛状癌 |
| 黏液癌 |
| 黏液性囊腺癌 |
| 浸润性微乳头状癌 |
| 伴大汗腺分化的癌 |
| 化生性癌 |
| 少见肿瘤和涎腺型肿瘤 |
| 腺泡细胞癌 |
| 腺样囊性癌 |
| 分泌性癌 |
| 黏液表皮样癌 |
| 多形性腺癌 |
| 伴有极性翻转的高细胞癌 |
| 神经内分泌肿瘤 |
| 神经内分泌瘤 |
| 神经内分泌癌 |
"
| 形态学特征 | 评分 | |||
|---|---|---|---|---|
| 腺管结构 | ||||
| 占肿瘤成分多数(>75%) | 1 | |||
| 中等数量(10% ~ 75%) | 2 | |||
| 少或无(<10%) | 3 | |||
| 细胞核的多形性 | ||||
| 细胞核小,形态规则一致 | 1 | |||
| 细胞核中等大小,不规则,大小不一 | 2 | |||
| 细胞核大,形态多样 | 3 | |||
| 核分裂象计数 | ||||
| 取决于镜下视野范围 | 1 ~ 3 | |||
| 3种不同视野范围核分裂象计数举例 | ||||
| 视野直径/mm | 0.44 | 0.55 | 0.63 | |
| 视野面积/mm2 | 0.152 | 0.237 | 0.312 | |
| 核分裂象计数(每10 HPF的核分裂象数目) | ||||
| 0 ~ 5 | 0 ~ 8 | 0 ~ 11 | 1 | |
| 6 ~ 11 | 9 ~ 17 | 12 ~ 22 | 2 | |
| ≥12 | ≥18 | ≥23 | 3 |
"
| 浸润性癌细胞核染色比例 | ER/PR判读标准 |
|---|---|
| 细胞核染色<1% | ER/PR阴性 |
| 细胞核染色1% ~ 10% | ER/PR阳性(低表达) |
| 细胞核染色>10% | ER/PR阳性 |
"
| 患者姓名:××× | 性别: | 年龄: | 送检日期: | 病理号: |
|---|---|---|---|---|
| 住院号: | 床号: | 科室: | 送检医师: | 标本类型: |
| 肉眼所见:(左乳)乳腺改良根治标本,乳腺大小27.0 cm×20.0 cm×3.5 cm。皮瓣面积19.0 cm×9.0 cm,乳头直径0.9 cm,高出皮肤0.3 cm,未见明显异常。内上象限,距乳头2.5 cm,皮下1.0 cm见大小约3.5 cm×3.0 cm×2.5 cm质硬肿块,切面灰白灰红、界限不清。查见腋窝淋巴结23枚,最大径0.5 ~ 1.2 cm。 | ||||
| 病理学诊断:(左乳)浸润性癌,非特殊类型,2级(腺管形成2分、核级2分、核分裂象2分,总分6分),伴导管原位癌(约占20%,中核级,粉刺样坏死,含钙化)。浸润癌最大径3.5 cm,可见脉管侵犯。周围乳腺呈乳头状瘤及腺病改变。乳头、乳腺表面皮肤及基底切缘均未见癌累及。腋窝淋巴结(7/23)查见癌转移。 | ||||
| 免疫组织化学检测提示浸润性癌:ER(+)(强,阳性细胞约70%)、PR(+)(中等强度,阳性细胞约60%)、HER2(0)、Ki-67增殖指数约30%。 | ||||
| 病理学分期:pT2N2Mx | ||||
| 报告医师签名: | ||||
| 审核医师签名: | ||||
| 报告日期: | ||||
VNPI"
| VNPI = A + B + C + D |
|---|
| A = 肿瘤大小 |
| 1:≤15 mm |
| 2:16~40 mm |
| 3:≥41 mm |
| B = 切缘情况 |
| 1:≥10 mm |
| 2:1~9 mm |
| 3:<1 mm |
| C = 细胞核分级 |
| 1:低级 |
| 2:中级 |
| 3:高级 |
| D = 年龄 |
| 1:≥60岁 |
| 2:40~59岁 |
| 3:<40岁 |
| [1] | WHO Classification of Tumours Editorial Board. Breast tumours[M]. 5th ed. Lyon: International Agency for Research on Cancer, 2019. |
| [2] | NCCN Clinical Practice Guideline in OncologyTM. Breast Cancer. 2014 National Comprehensive Cancer Network[EB/OL]. https://www.nccn.org/guidelines/nccn-guidelines/guidelines-detail?category=1&id=1419[2021-09-02]. |
| [3] | American Joint Committee on Cancer. AJCC cancer staging handbook[M]. 7th ed. Chicago: Springer, 2010. |
| [4] |
BUCHHOLZ T A, SOMERFIELD M R, GRIGGS J J, et al. Margins for breast-conserving surgery with whole-breast irradiation in stage Ⅰ and Ⅱ invasive breast cancer: American Society of Clinical Oncology endorsement of the Society of Surgical Oncology/American Society for Radiation Oncology consensus guideline[J]. J Clin Oncol, 2014, 32(14): 1502-1506.
doi: 10.1200/JCO.2014.55.1572 |
| [5] |
KUNKLER I H, WILLIAMS L J, JACK W J, et al. Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME Ⅱ): a randomised controlled trial[J]. Lancet Oncol, 2015, 16(3): 266-273.
doi: 10.1016/S1470-2045(14)71221-5 |
| [6] |
GIULIANO A E, MCCALL L, BEITSCH P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial[J]. Ann Surg, 2010, 252(3): 426-432; discussion 432-433.
doi: 10.1097/SLA.0b013e3181f08f32 pmid: 20739842 |
| [7] |
DONKER M, VAN TIENHOVEN G, STRAVER M E, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial[J]. Lancet Oncol, 2014, 15(12): 1303-1310.
doi: 10.1016/S1470-2045(14)70460-7 pmid: 25439688 |
| [8] |
MORAN M S, SCHNITT S J, GIULIANO A E, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages Ⅰ and Ⅱ invasive breast cancer[J]. J Clin Oncol, 2014, 32(14): 1507-1515.
doi: 10.1200/JCO.2013.53.3935 |
| [9] |
EARLY BREAST CANCER TRIALISTS' COLLABORATIVE GROUP EBCTCG. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials[J]. Lancet Oncol, 2018, 19(1): 27-39.
doi: S1470-2045(17)30777-5 pmid: 29242041 |
| [10] |
GIANNI L, PIENKOWSKI T, IM Y H, et al. 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial[J]. Lancet Oncol, 2016, 17(6): 791-800.
doi: S1470-2045(16)00163-7 pmid: 27179402 |
| [11] | SIKOV W M, BERRY D A, PEROU C M, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage Ⅱ to Ⅲ triple-negative breast cancer: CALGB 40603 (Alliance)[J]. J Clin Oncol, 2015, 33(1): 13-21. |
| [12] |
ADAMS S, LOI S, TOPPMEYER D, et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: cohort B of the phase Ⅱ KEYNOTE-086 study[J]. Ann Oncol, 2019, 30(3): 405-411.
doi: 10.1093/annonc/mdy518 |
| [13] |
ADAMS S, SCHMID P, RUGO H S, et al. Pembrolizumab monotherapy for previously treated metastatic triple-negative breast cancer: cohort A of the phase Ⅱ KEYNOTE-086 study[J]. Ann Oncol, 2019, 30(3): 397-404.
doi: 10.1093/annonc/mdy517 |
| [14] |
GOETZ M P, TOI M, CAMPONE M, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer[J]. J Clin Oncol, 2017, 35(32): 3638-3646.
doi: 10.1200/JCO.2017.75.6155 pmid: 28968163 |
| [15] |
ROBSON M, IM S A, SENKUS E, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation[J]. N Engl J Med, 2017, 377(6): 523-533.
doi: 10.1056/NEJMoa1706450 |
| [16] |
SLEDGE G W Jr, TOI M, NEVEN P, et al. MONARCH 2: abemaciclib in combination with fulvestrant in women with HR+/HER2- advanced breast cancer who had progressed while receiving endocrine therapy[J]. J Clin Oncol, 2017, 35(25): 2875-2884.
doi: 10.1200/JCO.2017.73.7585 pmid: 28580882 |
| [17] |
SCHMID P, ADAMS S, RUGO H S, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer[J]. N Engl J Med, 2018, 379(22): 2108-2121.
doi: 10.1056/NEJMoa1809615 |
| [18] |
TRIPATHY D, IM S A, COLLEONI M, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial[J]. Lancet Oncol, 2018, 19(7): 904-915.
doi: S1470-2045(18)30292-4 pmid: 29804902 |
| [19] |
TURNER N C, SLAMON D J, RO J, et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer[J]. N Engl J Med, 2018, 379(20): 1926-1936.
doi: 10.1056/NEJMoa1810527 |
| [20] | BLOK E J, KROEP J R, MEERSHOEK-KLEIN KRANENBARG E, et al. Optimal duration of extended adjuvant endocrine therapy for early breast cancer; results of the IDEAL trial (BOOG 2006-05)[J]. J Natl Cancer Inst, 2018, 110(1). |
| [21] |
BURSTEIN H J, LACCHETTI C, ANDERSON H, et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update[J]. J Clin Oncol, 2019, 37(5): 423-438.
doi: 10.1200/JCO.18.01160 pmid: 30452337 |
| [22] |
FRANCIS P A, PAGANI O, FLEMING G F, et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer[J]. N Engl J Med, 2018, 379(2): 122-137.
doi: 10.1056/NEJMoa1803164 |
| [23] |
GNANT M, MLINERITSCH B, STOEGER H, et al. Zoledronic acid combined with adjuvant endocrine therapy of tamoxifen versus anastrozol plus ovarian function suppression in premenopausal early breast cancer: final analysis of the Austrian Breast and Colorectal Cancer Study Group trial 12[J]. Ann Oncol, 2015, 26(2): 313-320.
doi: 10.1093/annonc/mdu544 pmid: 25403582 |
| [24] |
MAMOUNAS E P, BANDOS H, LEMBERSKY B C, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial[J]. Lancet Oncol, 2019, 20(1): 88-99.
doi: S1470-2045(18)30621-1 pmid: 30509771 |
| [25] |
METZGER FILHO O, GIOBBIE-HURDER A, MALLON E, et al. Relative effectiveness of letrozole compared with tamoxifen for patients with lobular carcinoma in the BIG 1-98 trial[J]. J Clin Oncol, 2015, 33(25): 2772-2779.
doi: 10.1200/JCO.2015.60.8133 pmid: 26215945 |
| [26] |
PAN H C, GRAY R, BRAYBROOKE J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years[J]. N Engl J Med, 2017, 377(19): 1836-1846.
doi: 10.1056/NEJMoa1701830 |
| [27] |
BLUM J L, FLYNN P J, YOTHERS G, et al. Anthracyclines in early breast cancer: the ABC trials-USOR 06-090, NSABP B-46-I/USOR 07132, and NSABP B-49 (NRG oncology)[J]. J Clin Oncol, 2017, 35(23): 2647-2655.
doi: 10.1200/JCO.2016.71.4147 pmid: 28398846 |
| [28] |
CARDOSO F, VAN'T VEER L J, BOGAERTS J, et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer[J]. N Engl J Med, 2016, 375(8): 717-729.
doi: 10.1056/NEJMoa1602253 |
| [29] |
EARLY BREAST CANCER TRIALISTS' COLLABORATIVE GROUP EBCTCG. Adjuvant bisphosphonate treatment in early breast cancer: meta-analyses of individual patient data from randomised trials[J]. Lancet, 2015, 386(10001): 1353-1361.
doi: S0140-6736(15)60908-4 pmid: 26211824 |
| [30] |
EARLY BREAST CANCER TRIALISTS' COLLABORATIVE GROUP EBCTCG. Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: a patient-level meta-analysis of 37 298 women with early breast cancer in 26 randomised trials[J]. Lancet, 2019, 393(10179): 1440-1452.
doi: 10.1016/S0140-6736(18)33137-4 |
| [31] |
LOIBL S, WEBER K E, TIMMS K M, et al. Survival analysis of carboplatin added to an anthracycline/taxane-based neoadjuvant chemotherapy and HRD score as predictor of response-final results from GeparSixto[J]. Ann Oncol, 2018, 29(12): 2341-2347.
doi: S0923-7534(19)34246-2 pmid: 30335131 |
| [32] |
MASUDA N, LEE S J, OHTANI S, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy[J]. N Engl J Med, 2017, 376(22): 2147-2159.
doi: 10.1056/NEJMoa1612645 |
| [33] |
MOORE H C, UNGER J M, PHILLIPS K A, et al. Goserelin for ovarian protection during breast-cancer adjuvant chemotherapy[J]. N Engl J Med, 2015, 372(10): 923-932.
doi: 10.1056/NEJMoa1413204 |
| [34] |
NITZ U, GLUZ O, CLEMENS M, et al. West German study PlanB trial: adjuvant four cycles of epirubicin and cyclophosphamide plus docetaxel versus six cycles of docetaxel and cyclophosphamide in HER2-negative early breast cancer[J]. J Clin Oncol, 2019, 37(10): 799-808.
doi: 10.1200/JCO.18.00028 pmid: 30785826 |
| [35] |
SPARANO J A, GRAY R J, MAKOWER D F, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer[J]. N Engl J Med, 2018, 379(2): 111-121.
doi: 10.1056/NEJMoa1804710 |
| [36] |
PROWELL T M, BEAVER J A, PAZDUR R. Residual disease after neoadjuvant therapy - developing drugs for high-risk early breast cancer[J]. N Engl J Med, 2019, 380(7): 612-615.
doi: 10.1056/NEJMp1900079 |
| [37] |
SPARANO J A, GRAY R J, RAVDIN P M, et al. Clinical and genomic risk to guide the use of adjuvant therapy for breast cancer[J]. N Engl J Med, 2019, 380(25): 2395-2405.
doi: 10.1056/NEJMoa1904819 |
| [38] |
EARL H M, HILLER L, VALLIER A L, et al. 6 versus 12 months of adjuvant trastuzumab for HER2-positive early breast cancer (PERSEPHONE): 4-year disease-free survival results of a randomised phase 3 non-inferiority trial[J]. Lancet, 2019, 393(10191): 2599-2612.
doi: S0140-6736(19)30650-6 pmid: 31178152 |
| [39] |
MARTIN M, HOLMES F A, EJLERTSEN B, et al. Neratinib after trastuzumab-based adjuvant therapy in HER2-positive breast cancer (ExteNET): 5-year analysis of a randomised, double-blind, placebo-controlled, phase 3 trial[J]. Lancet Oncol, 2017, 18(12): 1688-1700.
doi: S1470-2045(17)30717-9 pmid: 29146401 |
| [40] |
VON MINCKWITZ G, HUANG C S, MANO M S, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer[J]. N Engl J Med, 2019, 380(7): 617-628.
doi: 10.1056/NEJMoa1814017 |
| [41] |
VON MINCKWITZ G, PROCTER M, DE AZAMBUJA E, et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer[J]. N Engl J Med, 2017, 377(2): 122-131.
doi: 10.1056/NEJMoa1703643 |
| [42] |
GIANNI L, PIENKOWSKI T, IM Y H, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial[J]. Lancet Oncol, 2012, 13(1): 25-32.
doi: 10.1016/S1470-2045(11)70336-9 pmid: 22153890 |
| [43] |
MA F, LI Q, CHEN S S, et al. Phase I study and biomarker analysis of pyrotinib, a novel irreversible pan-ErbB receptor tyrosine kinase inhibitor, in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer[J]. J Clin Oncol, 2017, 35(27): 3105-3112.
doi: 10.1200/JCO.2016.69.6179 pmid: 28498781 |
| [44] |
LANG G T, JIANG Y Z, SHI J X, et al. Characterization of the genomic landscape and actionable mutations in Chinese breast cancers by clinical sequencing[J]. Nat Commun, 2020, 11(1): 5679.
doi: 10.1038/s41467-020-19342-3 |
| [45] |
JIANG Y Z, MA D, SUO C, et al. Genomic and transcriptomic landscape of triple-negative breast cancers: subtypes and treatment strategies[J]. Cancer Cell, 2019, 35(3): 428-440.e5.
doi: 10.1016/j.ccell.2019.02.001 |
| [46] |
LI J J, YU K D, PANG D, et al. Adjuvant capecitabine with docetaxel and cyclophosphamide plus epirubicin for triple-negative breast cancer (CBCSG010): an open-label, randomized, multicenter, phase Ⅲ trial[J]. J Clin Oncol, 2020, 38(16): 1774-1784.
doi: 10.1200/JCO.19.02474 |
| [47] |
YU K D, YE F G, HE M, et al. Effect of adjuvant paclitaxel and carboplatin on survival in women with triple-negative breast cancer: a phase 3 randomized clinical trial[J]. JAMA Oncol, 2020, 6(9): 1390-1396.
doi: 10.1001/jamaoncol.2020.2965 |
| [48] |
WANG X, WANG S S, HUANG H, et al. Effect of capecitabine maintenance therapy using lower dosage and higher frequency vs observation on disease-free survival among patients with early-stage triple-negative breast cancer who had received standard treatment: the SYSUCC-001 randomized clinical trial[J]. JAMA, 2021, 325(1): 50-58.
doi: 10.1001/jama.2020.23370 |
| [49] |
HU X C, ZHANG J, XU B H, et al. Cisplatin plus gemcitabine versus paclitaxel plus gemcitabine as first-line therapy for metastatic triple-negative breast cancer (CBCSG006): a randomised, open-label, multicentre, phase 3 trial[J]. Lancet Oncol, 2015, 16(4): 436-446.
doi: 10.1016/S1470-2045(15)70064-1 |
| [50] |
ZHANG J, LIN Y, SUN X J, et al. Biomarker assessment of the CBCSG006 trial: a randomized phase Ⅲ trial of cisplatin plus gemcitabine compared with paclitaxel plus gemcitabine as first-line therapy for patients with metastatic triple-negative breast cancer[J]. Ann Oncol, 2018, 29(8): 1741-1747.
doi: 10.1093/annonc/mdy209 |
| [51] |
LIN M X, CHEN Y, JIN Y Z, et al. Comparative overall survival of CDK4/6 inhibitors plus endocrine therapy vs endocrine therapy alone for hormone receptor-positive, HER2-negative metastatic breast cancer[J]. J Cancer, 2020, 11(24): 7127-7136.
doi: 10.7150/jca.48944 |
| [52] |
FALLON M, GIUSTI R, AIELLI F, et al. Management of cancer pain in adult patients: ESMO clinical practice guidelines[J]. Ann Oncol, 2018, 29(Suppl 4): iv166-iv191.
doi: 10.1093/annonc/mdy152 |
| [53] |
ZHAO S, MA D, XIAO Y, et al. Molecular subtyping of triple-negative breast cancers by immunohistochemistry: molecular basis and clinical relevance[J]. Oncologist, 2020, 25(10): e1481-e1491.
doi: 10.1634/theoncologist.2019-0982 |
| [54] |
JIANG Y Z, LIU Y, XIAO Y, et al. Molecular subtyping and genomic profiling expand precision medicine in refractory metastatic triple-negative breast cancer: the FUTURE trial[J]. Cell Res, 2021, 31(2): 178-186.
doi: 10.1038/s41422-020-0375-9 |
| [55] |
ALBABTAIN H, ALWHAIBI M, ALBURAIKAN K, et al. Quality of life and complementary and alternative medicine use among women with breast cancer[J]. Saudi Pharm J, 2018, 26(3): 416-421.
doi: 10.1016/j.jsps.2017.12.020 pmid: 29556133 |
| [56] | 林洪生, 刘杰, 张英. 《恶性肿瘤中医诊疗指南》的内涵及其意义[J]. 中国肿瘤临床与康复, 2016, 23(3): 257-260. |
| LIN H S, LIU J, ZHANG Y. Connotation and significance of “Guidelines for Diagnosis and Treatment of Malignant Tumors in Traditional Chinese Medicine”[J]. Chin J Clin Oncol Rehabil, 2016, 23(3): 257-260. | |
| [57] | 陈前军, 裴晓华. 早期乳腺癌中医辨证内治专家共识[J]. 现代中医临床, 2020, 27(3): 5-8. |
| CHEN Q J, PEI X H. Consensus on TCM syndrome differentiation and internal therapy for early-stage breast cancer[J]. Mod Chin Clin Med, 2020, 27(3): 5-8. | |
| [58] | 杨雯靖, 念家云, 杨国旺. 中西医结合治疗乳腺癌现状及展望[J]. 北京中医药, 2020, 39(10): 1009-1013. |
| YANG W J, NIAN J Y, YANG G W. Present situation and prospect of treating breast cancer with integrated traditional Chinese and western medicine[J]. Beijing J Tradit Chin Med, 2020, 39(10): 1009-1013. | |
| [59] | 马瑞, 张丹, 林从尧. 小金丸、逍遥丸及乳癖散结胶囊治疗乳腺增生的临床观察[J]. 现代中西医结合杂志, 2015, 24(2): 140-142. |
| MA R, ZHANG D, LIN C Y. Clinical observation of Koganemaru, Xiaoyao Pill and Rubisanjie Capsule in the treatment of mammary hyperplasia[J]. Mod J Integr Tradit Chin West Med, 2015, 24(2): 140-142. | |
| [60] | 《乳腺癌HER检测指南版》编写组. 《乳腺癌HER2检测指南(2019版)》[J]. 中华病理学杂志, 2019, 48(3): 169-175. |
| HER2 Detection Guidline for Breast Cancer (2019 Edition) Writing Group. HER2 guideline for breast cancer (2019 Edition)[J]. Chin J Pathol, 2019, 48(3): 169-175. | |
| [61] | 《乳腺癌新辅助治疗的病理诊断专家共识2020版》编写组. 乳腺癌新辅助治疗的病理诊断专家共识(2020版)[J]. 中华病理学杂志, 2020, 49(4): 296-304. |
| Expert Consensus on Pathological Diagnosis of Neoadjuvant Therapy for Breast Cancer (2020 Edition) Writing Group. Writing Group. Expert consensus on pathological diagnosis of neoadjuvant therapy for breast cancer (2020 Edition)[J]. Chin J Pathol, 2020, 49(4): 296-304. | |
| [62] | 《乳腺癌雌、孕激素受体检测指南》编写组. 乳腺癌雌、孕激素受体检测指南[J]. 中华病理学杂志, 2015, 44(4): 237-240. |
| Guidelines for Detection of Estrogen and Progesterone Receptors in Breast Cancer Writing Group. Guidelines for detection of estrogen and progesterone receptors in breast cancer[J]. Chin J Pathol, 2015, 44(4): 237-240. | |
| [63] |
GOLDHIRSCH A, INGLE J N, GELBER R D, et al. Thresholds for therapies: highlights of the St Gallen International Expert Consensus on the primary therapy of early breast cancer 2009[J]. Ann Oncol, 2009, 20(8): 1319-1329.
doi: 10.1093/annonc/mdp322 pmid: 19535820 |
| [64] |
GOLDHIRSCH A, WOOD W C, COATES A S, et al. Strategies for subtypes: dealing with the diversity of breast cancer: highlights of the St. Gallen international expert consensus on the primary therapy of early breast cancer 2011[J]. Ann Oncol, 2011, 22(8): 1736-1747.
doi: 10.1093/annonc/mdr304 |
| [65] |
GOLDHIRSCH A, WINER E P, COATES A S, et al. Personalizing the treatment of women with early breast cancer: highlights of the St. Gallen international expert consensus on the primary therapy of early breast cancer 2013[J]. Ann Oncol, 2013, 24(9): 2206-2223.
doi: 10.1093/annonc/mdt303 pmid: 23917950 |
| [66] |
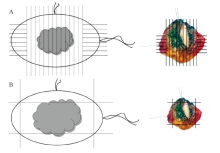
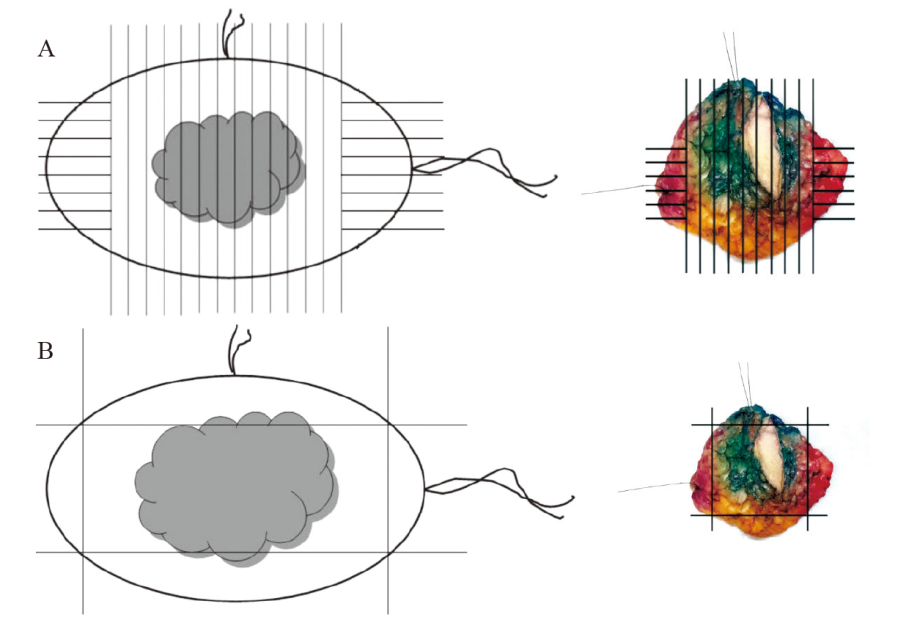
WRIGHT M J, PARK J, FEY J V, et al. Perpendicular inked versus tangential shaved margins in breast-conserving surgery: does the method matter?[J]. J Am Coll Surg, 2007, 204(4): 541-549.
doi: 10.1016/j.jamcollsurg.2007.01.031 |
| [67] |
ELSTON C W, ELLIS I O. Pathological prognostic factors in breast cancer.Ⅰ. The value of histological grade in breast cancer: experience from a large study with long-term follow-up[J]. Histopathology, 2002, 41(3a): 154-161.
doi: 10.1046/j.1365-2559.2002.14892.x |
| [68] |
FRIERSON H F Jr, WOLBER R A, BEREAN K W, et al. Interobserver reproducibility of the Nottingham modification of the Bloom and Richardson histologic grading scheme for infiltrating ductal carcinoma[J]. Am J Clin Pathol, 1995, 103(2): 195-198.
doi: 10.1093/ajcp/103.2.195 pmid: 7856562 |
| [69] |
HAMMOND M E, HAYES D F, DOWSETT M, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer[J]. Arch Pathol Lab Med, 2010, 134(6): 907-922.
doi: 10.1043/1543-2165-134.6.907 pmid: 20524868 |
| [70] |
DOWSETT M, NIELSEN T O, A’HERN R, et al. Assessment of Ki-67 in breast cancer: recommendations from the international Ki-67 in breast cancer working group[J]. J Natl Cancer Inst, 2011, 103(22): 1656-1664.
doi: 10.1093/jnci/djr393 |
| [71] |
WOLFF A C, HAMMOND M E, HICKS D G, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update[J]. J Clin Oncol, 2013, 31(31): 3997-4013.
doi: 10.1200/JCO.2013.50.9984 pmid: 24101045 |
| [72] |
SYMMANS W F, PEINTINGER F, HATZIS C, et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy[J]. J Clin Oncol, 2007, 25(28): 4414-4422.
doi: 10.1200/JCO.2007.10.6823 pmid: 17785706 |
| [73] |
OGSTON K N, MILLER I D, PAYNE S, et al. A new histological grading system to assess response of breast cancers to primary chemotherapy: prognostic significance and survival[J]. Breast, 2003, 12(5): 320-327.
doi: 10.1016/s0960-9776(03)00106-1 pmid: 14659147 |
| [74] | 水若鸿, 杨文涛. 乳腺癌Ki-67阳性指数的检测和评估[J]. 中华病理学杂志, 2013, 42(6): 420-423. |
| SHUI R H, YANG W T. Detection and evaluation of Ki-67 positive index in breast cancer[J]. Chin J Pathol, 2013, 42(6): 420-423. | |
| [75] | LIN M X, JIN Y Z, YANG Z Y, et al. Determination and clinical significance of bone pseudoprogression in hormone receptor-positive metastatic breast cancer[J]. Ther Adv Med Oncol, 2021, 13: 17588359211022881. |
| [76] |
ZHANG J F, LIN M X, JIN Y Z, et al. Cisplatin given at three divided doses for three consecutive days in metastatic breast cancer: an alternative schedule for one full dose with comparable efficacy but less CINV and hypomagnesaemia[J]. Breast Cancer Res Treat, 2020, 182(3): 719-726.
doi: 10.1007/s10549-020-05730-2 |
| [77] | 《肿瘤病理诊断规范》项目组. 肿瘤病理诊断规范(乳腺癌)[J]. 中华病理学杂志 2016, 45(8): 525-528. |
| The project team of Tumor Pathological Diagnosis Standard. Diagnostic criteria for tumor pathology (breast cancer)[J]. Chin J Pathol, 2016, 45 (8): 525-528. | |
| [78] | 《中国乳腺导管原位癌病理诊断共识2022版》编写组. 中国乳腺导管原位癌病理诊断共识(2022版)[J]. 中华病理学杂志, 2022, 51(9): 812-818. |
| The Writing Team of the Chinese Consensus on Pathological Diagnosis of Breast Ductal Carcinoma in situ (2022 Edition). Chinese consensus on pathological diagnosis of ductal carcinoma in situ of the breast (2022 edition)[J]. Chin J Pathol, 2022, 51 (9): 812-818. | |
| [79] | 杨昭志, 孟晋, 马金利, 等. 早期乳腺癌术后靶区勾画共识[J]. 中国癌症杂志, 2019, 29(9): 753-760. |
| YANG Z Z, MENG J, MA J L, et al. Early stage breast cancer postoperative target volume contouring[J]. China Oncol, 2019, 29(9)753-760 | |
| [80] |
WOLFF A C, ELIZABETH HALE HAMMOND M, ALLISON K H, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update[J]. J Clin Oncol, 2018, 36(20): 2105-2122.
doi: 10.1200/JCO.2018.77.8738 pmid: 29846122 |
| [81] |
WOLFF A C, SOMERFIELD M R, DOWSETT M, et al. Human epidermal growth factor receptor 2 testing in breast cancer: ASCO-College of American Pathologists guideline update[J]. J Clin Oncol, 2023, 41(22): 3867-3872.
doi: 10.1200/JCO.22.02864 |
| [82] |
TARANTINO P, VIALE G, PRESS M F, et al. ESMO expert consensus statements (ECS) on the definition, diagnosis, and management of HER2-low breast cancer[J]. Ann Oncol, 2023, 34(8): 645-659.
doi: 10.1016/j.annonc.2023.05.008 pmid: 37269905 |
| [83] |
SHI F, LIANG Z, ZHANG Q, et al. The performance of one-step nucleic acid amplification assay for intraoperative detection of sentinel lymph node macrometastasis in breast cancer: an updated meta-analysis[J]. Breast, 2018, 39: 39-45.
doi: S0960-9776(18)30053-5 pmid: 29574393 |
| [84] | HUXLEY N, JONES-HUGHES T, COELHO H, et al. Intraoperative tests (RD-100i OSNA system and Metasin test) for detecting sentinel lymph node metastases in breast cancer[J]. Health Technol Assess, 2015, 19(2): Ⅴ-ⅩⅩⅤ. |
| [85] | BUNDRED J R, MICHAEL S, STUART B, et al. Margin status and survival outcomes after breast cancer conservation surgery: prospectively registered systematic review and meta-analysis[J]. BMJ, 2022, 378: e070346. |
| [86] | 中国抗癌协会乳腺癌专业委员会. 中国抗癌协会乳腺癌诊治指南与规范(2021年版)[J]. 中国癌症杂志, 2021, 31(10): 954-1040. |
| The Society of Breast Cancer China Anti-Cancer Association. Guidelines for breast cancer diagnosis and treatment by China Anti-cancer Association (2021 edition)[J]. China Oncol, 2021, 31(10): 954-1040. |
| [1] | XU Rui, WANG Zehao, WU Jiong. Advances in the role of tumor-associated neutrophils in the development of breast cancer [J]. China Oncology, 2024, 34(9): 881-889. |
| [2] | CAO Xiaoshan, YANG Beibei, CONG Binbin, LIU Hong. The progress of treatment for brain metastases of triple-negative breast cancer [J]. China Oncology, 2024, 34(8): 777-784. |
| [3] | Cancer Assessment Society of China Anti-Cancer Association, Cancer Pain Society of Fujian Anti-Cancer Association. Chinese expert consensus on whole-process management of oxaliplatin-induced hypersensitivity reactions (2024 edition) [J]. China Oncology, 2024, 34(8): 785-805. |
| [4] | ZHANG Jian. Clinical consideration of two key questions in assessing menopausal status of female breast cancer patients [J]. China Oncology, 2024, 34(7): 619-627. |
| [5] | JIANG Dan, SONG Guoqing, WANG Xiaodan. Study on the mechanism of mitochondrial dysfunction and CPT1A/ERK signal transduction pathway regulating malignant behavior in breast cancer [J]. China Oncology, 2024, 34(7): 650-658. |
| [6] | LIU Shuai, ZHANG Kai, ZHANG Xiaoqing, LUAN Wei. An exploratory study on the perioperative treatment of locally advanced gastric cancer with combination of penpulimab, anlotinib and chemotherapy [J]. China Oncology, 2024, 34(7): 659-668. |
| [7] | DONG Jianqiao, LI Kunyan, LI Jing, WANG Bin, WANG Yanhong, JIA Hongyan. A study on mechanism of SIRT3 inducing endocrine drug resistance in breast cancer via deacetylating YME1L1 [J]. China Oncology, 2024, 34(6): 537-547. |
| [8] | HAO Xian, HUANG Jianjun, YANG Wenxiu, LIU Jinting, ZHANG Junhong, LUO Yubei, LI Qing, WANG Dahong, GAO Yuwei, TAN Fuyun, BO Li, ZHENG Yu, WANG Rong, FENG Jianglong, LI Jing, ZHAO Chunhua, DOU Xiaowei. Establishment of primary breast cancer cell line as new model for drug screening and basic research [J]. China Oncology, 2024, 34(6): 561-570. |
| [9] | CHEN Hong, CAO Zhiyun. Recent progress in the construction and application of patient-derived pancreatic cancer organoid models [J]. China Oncology, 2024, 34(6): 590-597. |
| [10] | Urologic Chinese Oncology Group. Expert consensus on early diagnosis and treatment of bladder cancer (2024 edition) [J]. China Oncology, 2024, 34(6): 607-618. |
| [11] | Professional Committee on Gastric Cancer of Shanghai Anticancer Association , Professional Committee on Gastrointestinal Cancer of China Association for Promotion of Health Science and Technology . Chinese expert consensus on clinical practice of locally advanced gastric cancer invading adjacent organs (2024 edition) [J]. China Oncology, 2024, 34(5): 517-526. |
| [12] | FENG Zheng, GUO Qinhao, ZHU Jun, WU Xiaohua, WEN Hao. Progress in treatment of gynecological cancer in 2023 [J]. China Oncology, 2024, 34(4): 340-360. |
| [13] | MA Fenghua, JIANG Anqi, CHEN Yiqing, XU Congjian, KANG Yu. Magnetic resonance imaging for distinguishing gastric-type endocervical adenocarcinoma from lobular endocervical glandular hyperplasia [J]. China Oncology, 2024, 34(4): 380-388. |
| [14] | XU Yonghu, XU Dazhi. Progress and prospects of gastric cancer treatment in the 21st century [J]. China Oncology, 2024, 34(3): 239-249. |
| [15] | WANG Xuefei, ZHOU Peng, TANG Zhaoqing. New progress and development trend of surgical treatment for gastric cancer [J]. China Oncology, 2024, 34(3): 250-258. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
沪ICP备12009617
Powered by Beijing Magtech Co. Ltd